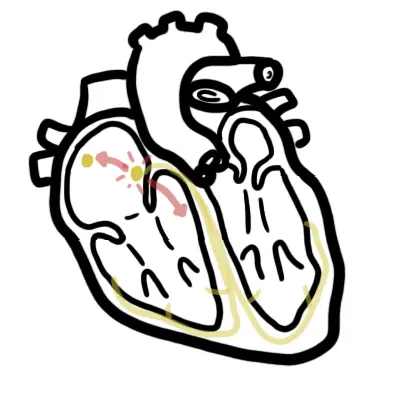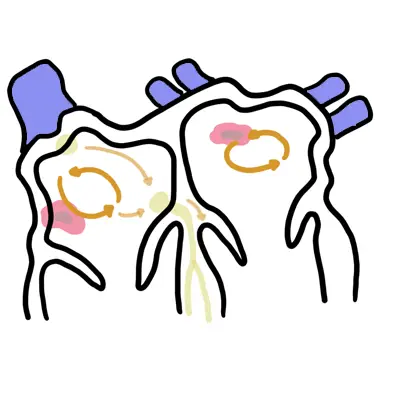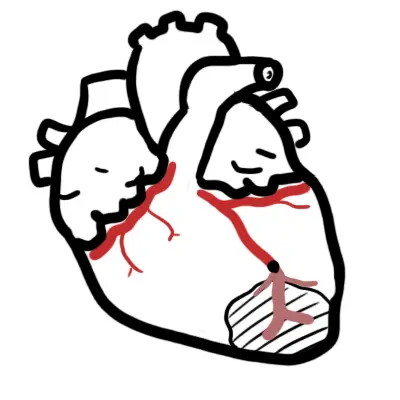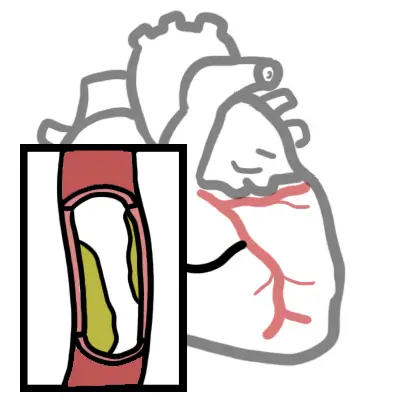
Overview Angina Pectoris refers to the pain caused by myocardial ischaemia. Myocardial Ischaemia is usually caused by stenosis within the vessel decreasing blood flow to the muscle, but it can be caused by tachycardia, anaemia, aortic stenosis, left ventricular hypertophy and many other disease. Angina "latin choking".
| Definitions Angina Pectoris: Pain caused by myocardial ischaemia (not myocardial infarction) Acute myocardial Infarction: Death of myocardial tissue because of inadequate blood flow Acute coronary Syndrome: Coronary artery obstruction or rupture can result in a variety of ischaemic condition which fall under the term of acute coronary syndrome. This does not include stable angina. Unstable angina is defined by the absence of biochemical evidence of myocardial damage. It is characterised by specific clinical findings of prolonged (>20 minutes) angina at rest; new onset of severe angina; angina that is increasing in frequency, longer in duration, or lower in threshold; or angina that occurs after a recent episode of MI. |
| Modifiable | Non-modifiable |
| Smoking | Increasing age |
| Hypertension | Male sex |
| Dyslipidaemia | Family history |
| Diabetes mellitus | Ethnicity |
| Obesity | |
| Physical inactivity | |
| High calorie intake diet | |
| Psychological stress |
Angina is classified according to its temporal pattern and its relation to exertion
| Remember Unstable Angina is part of Acute Coronary syndrome. Stable angina is NOT part of acute coronary syndrome |
Rule out acute coronary syndrome if presenting to Emergency. Stable angina chest pain typically resolves with rest.
| Remember Myocardial Ischaemia will respond to nitrates almost immediately |
| Think Chest wall tenderness suggests musculoskeletal pain and does not accompany angina |
| CAUSES OF CHEST PAIN BY BODY SYSTEMS | ||||
| Cardiac | Respiratory | Gastrointestinal | Musculoskeletal | Psychogenic |
| Acute Coronary Syndrome | Pulmonary Embolism | Oesophageal rupture | Rib Fracture | Anxiety |
| Aortic dissection | Pneumothorax | Pneumomediastinum | Herpes Zoster | Panic attack |
| Pericarditis | Pulmonary Hypertension | Cholecystitis | Costochondritis | |
| Stable Angina | Pneumonia | GERD | ||
| Endocarditis | Lung Cancer | Peptic ulcer disease | ||
| Cardiac tamponade | Bronchiectasis | Acute Pancreatitis | ||
Test to induce ischaemic chest pain
Non-pharmacological
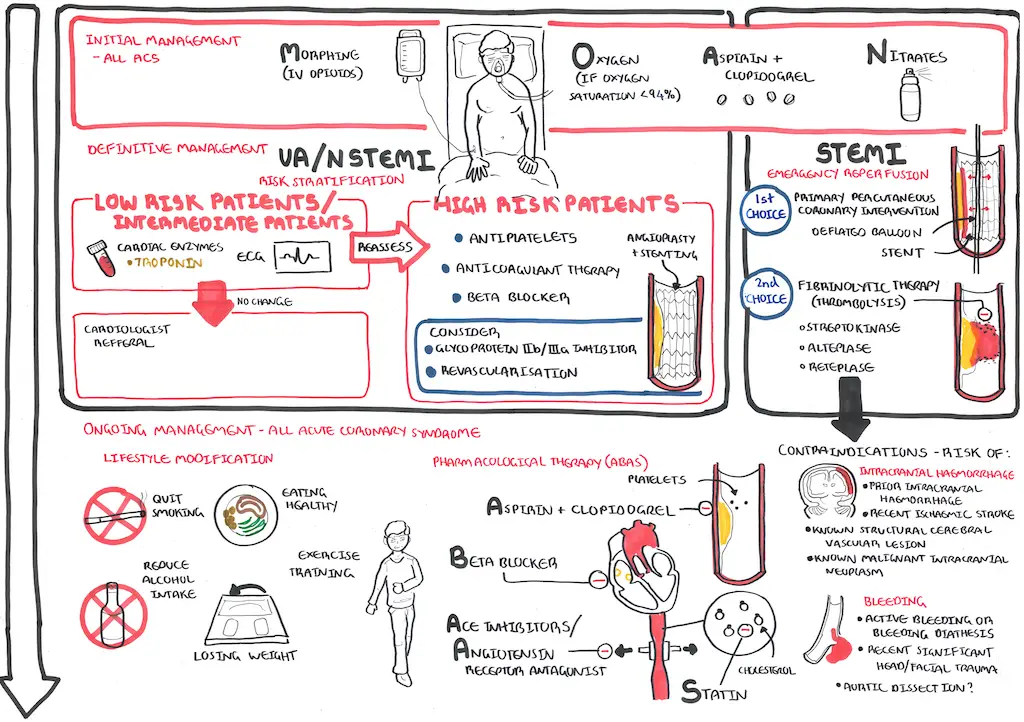
Pharmacological (BANS)
| Pharmacology Aspirin is a COX 1/2 inhibitor. It prevents the production of Prostagladins (inflammation: fever and pain) and thromboxane (clotting). It is used to treat fever, osteoarthritis, heart conditions and stroke. Side effects: nausea/vomiting, dyspepsia, stomach ulcer or bleeding problems, headache, dizziness, tinnitus, renal dysfunction and Reye’s syndrome (particularly in children who have taken aspirin) |
| Pharmacology Statins are competitive HMG-CoA reductase inhibitors, an enzyme normally responsible for producing cholesterol. By lowering the levels, they help prevent heart attacks and stroke. Side effects: Headache, difficulty sleeping, flushing of the skin, myalgia, liver enzyme dysfunction, nausea or vomiting, abdominal cramping or pain, bloating or gas and serious cases myositis and Rhabdomyolysis |
| Watch Video Acute Coronary Syndrome |