Overview Complex chronic syndrome characterised by recurrent abdominal pain and bowel dysfunction, in the absence of a structural abnormality. It is not associated with an increase in mortality, however, it is associated with substantial morbidity and a significant decrease in an individual’s quality of life.
| Definitions IBS IBD |
IBS belongs to a group of disorders collectively known as Functional Gastrointestinal Disorders. Functional Gastrointestinal Disorders are disorders of the digestive system where symptoms occur without structural or tissue abnormality. IBS is more common in Females (Female to Male Ratio = 2:1). There is a 2 fold increase in the prevalence of IBS among individuals who have relatives affected by IBS.
Side note Other Functional Gastrointestinal Disorders:
|
The population prevalence of IBS is high (∼11%) and the condition has considerable consequences for quality of life (QOL) that are comparable to other chronic diseases, such as diabetes mellitus and hepatitis.
General
| Classic Triad: Abdominal pain, diarrhea, and constipation. |
IBS is often associated with other somatic comorbidities (for example, pain syndromes, overactive bladder and migraine), psychiatric conditions (including depression and anxiety) and visceral sensitivity.
Red flags
Diagnosis
Diagnostic criteria for irritable bowel syndrome (IBS) include recurrent abdominal pain or discomfort at least 3 days per month in the past 3 months associated with two or more of the following:
These changes have to be present at least 6 months after onset of symptoms
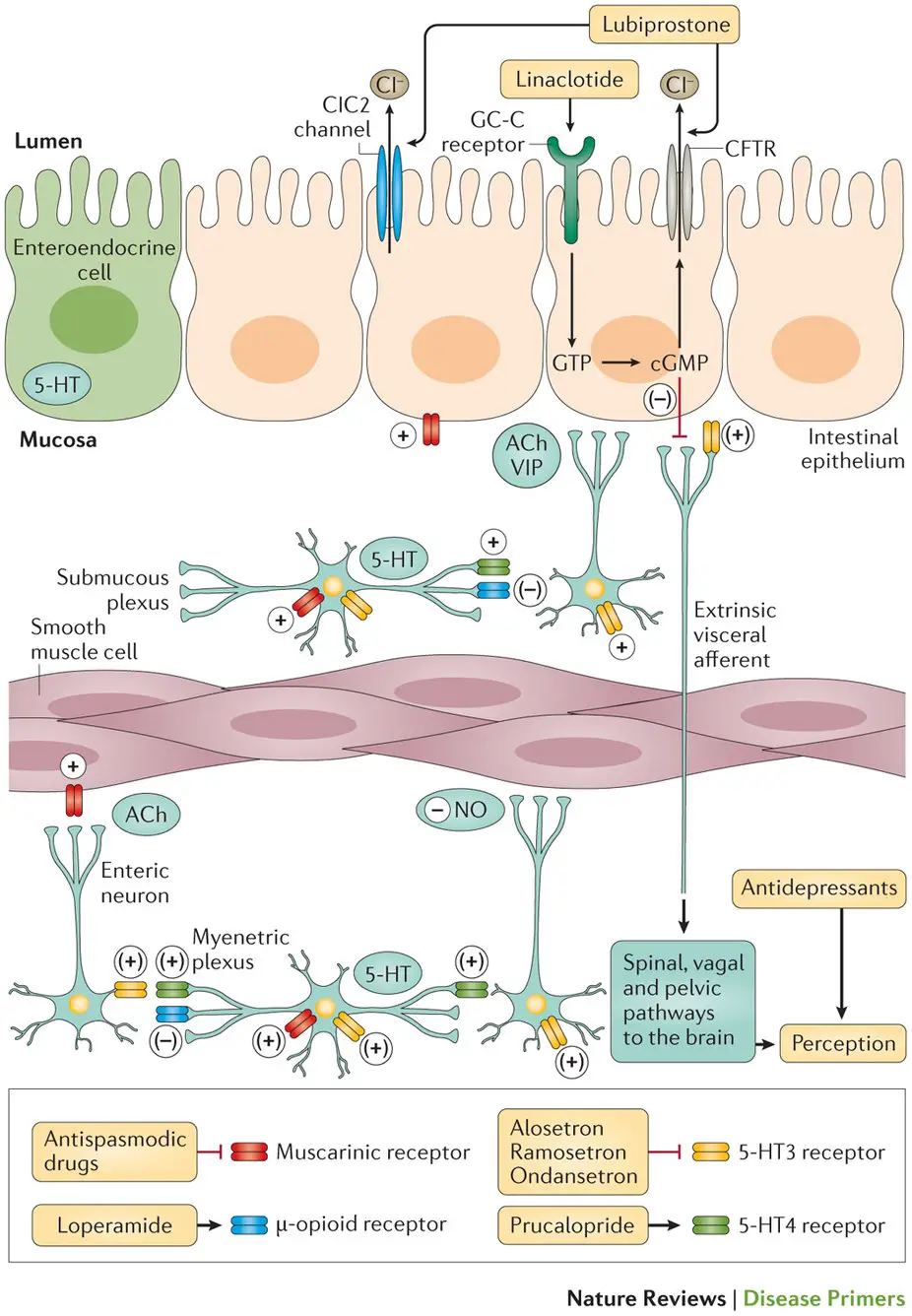
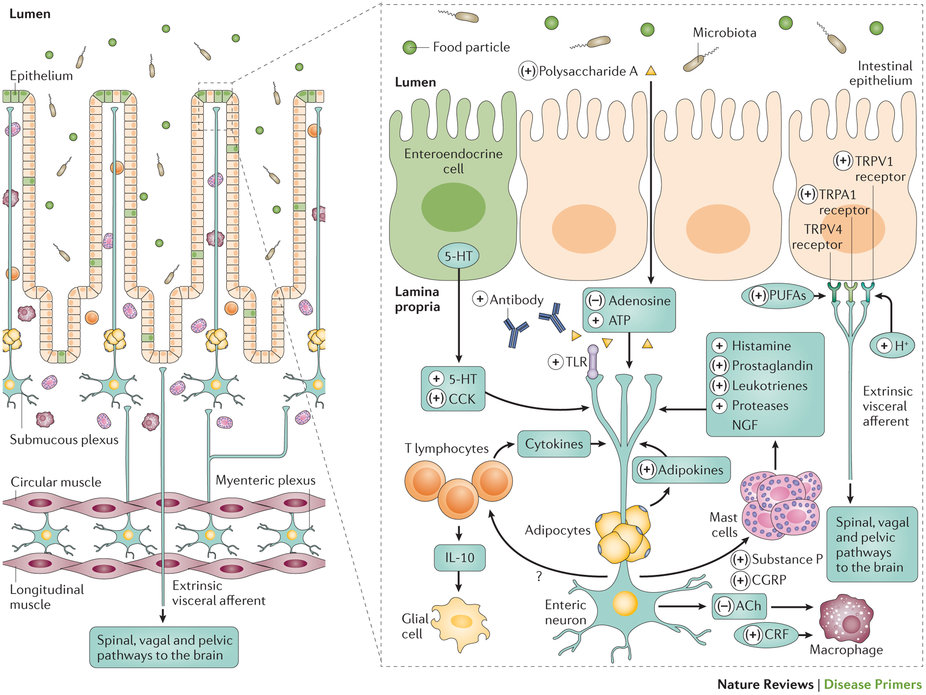
The pathophysiology of IBS is unclear. There are no specific anatomical, endoscopic, microbiological or histological findings that indicate a clear pathophysiology.
According to current understanding, IBS arises due to multiple factors that contribute to alteration of:
Only a fraction of patients with IBS-like symptoms (∼50%) seek medical care