The successful transition from intrauterine to extrauterine life is dependent upon significant physiologic changes that occur at birth.
Infants who are more likely to require resuscitation can be identified by the presence of one or more of the following risk factors:
Initial care steps in the delivery room are started within a few seconds of birth and should be applied throughout resuscitation
Initial Step
1. Identify risks and prepare resuscitation bay before delivery. Prewarm the bay and make sure oxygen and suction tubes are working.
2. Maintain temperature: Hypothermia in the newborn is associated with increase mortality. Maintaining heat by placing baby under a prewarmed heat source and wrapped around towel is important. Low birth weight and preterm infants are particularly prone to rapid loss of body heat because of their large body surface area relative to their mass, thin skin, and decreased subcutaneous fat.
3. Stimulation: Tactile stimulation of the newborn should be initiated promptly after birth. Tactile stimulation helps infant take their first breath
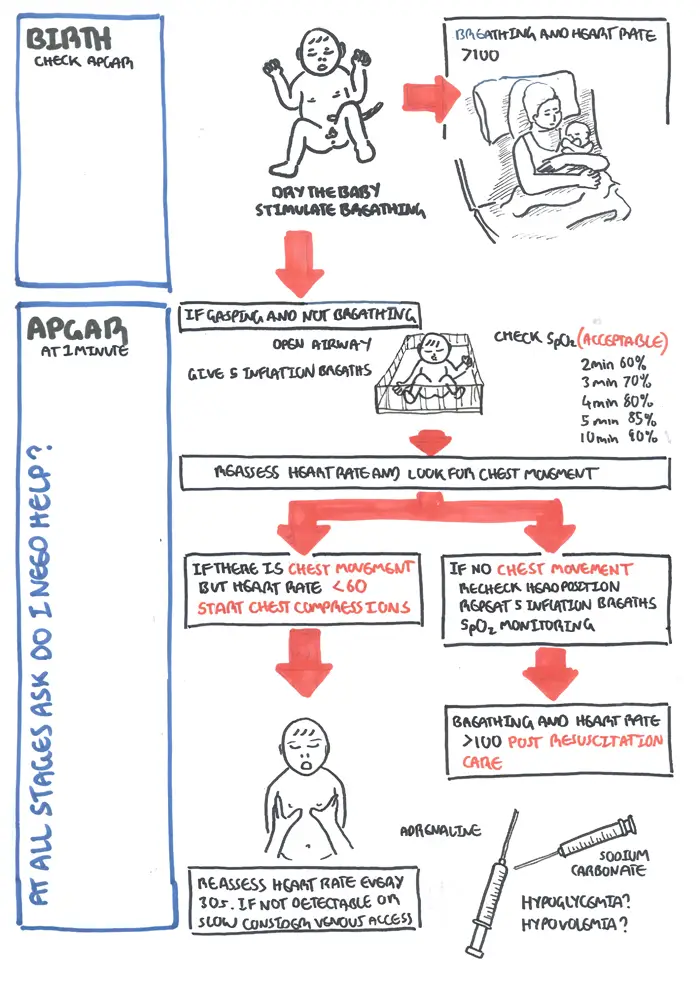
4. Assess infant heart rate, breathing and muscle tone (calculate APGAR as you go along at 1 and 5 min)
If Neonate is not breathing and gasping for air (or low heart rate and appear lifeless)
| Remember: At all stages ask "do I need help?" |
1. Airway: Check for clear airways. Place infant down with back flat in a neutral position, do not hyperextend the neck. Suctioning is reserved for clear obstruction. Wiping and suctioning of mouth first and nose second can be performed if fluid is present.
2. Heart Rate and vitals: Assess heart rate (this can be done on the umbilical cord or apex of heart), if below <100bpm check oxygen saturation and consider CPR. Monitor oxygen saturation and other vital signs as you go along.
3. Check for chest expansion
| Acceptable pre-ductal SpO2 |
| 2 min ~60% |
| 3 min ~70% |
| 4 min ~80% |
| 5 min ~85% |
| 10 min ~90% |
Next Steps
1. Oxygen
2. Positive pressure ventilation
3. CPAP in very preterm infants at risk for respiratory distress syndrome (RDS) with spontaneous ventilation is the preferred intervention versus the combined regimen of endotracheal intubation, surfactant therapy, and mechanical ventilation
4. Chest compression if heart rate is not detectable or slow, <60bpm (3 compression to 1 breath). Repeat and reassess infant every 30 seconds
| Remember: Reassess heart rate every 30s if heart is not detectable or slow consider venous access and drugs |
5. Medication including adrenaline (0.1ml/kg), sodium bicarbonate (1-2mmol/kg), 10% glucose bolus if hypoglycemic (2.5ml/kg). Atropine and calcium have no role in newborn resuscitation.
6. Endotracheal Intubation?