Overview Acute kidney injury (AKI) (formerly acute renal failure) is the syndrome arising from a rapid fall in GFR (over hours to days). It is characterized by retention of both nitrogenous (including Urea and Creatinine) and non-nitrogenous waste products of metabolism, as well as disordered electrolyte, acid– base, and fluid homeostasis.
| Remember AKI is neither a diagnosis nor a disease. Rather, it is a clinical syndrome that is caused by, or complicates, a wide range of disorders |
| Definition Acute Kidney Injury: Rapid reduction in kidney function over hours to days, as measured by serum urea and creatinine and leading to a failure to maintain fluid, electrolyte and acid-base homeostasis. Chronic Kidney Disease: Impaired renal function >3months based on abnormal structure or function, or GFR <60 for >3months. Oliguria: A urine output of <400ml/day may be the earlier sign of impaired renal function |
Epidemiology
Develop in 5- 20% of hospitalised patients and a significant contributor to morbidity and mortality in the critically ill
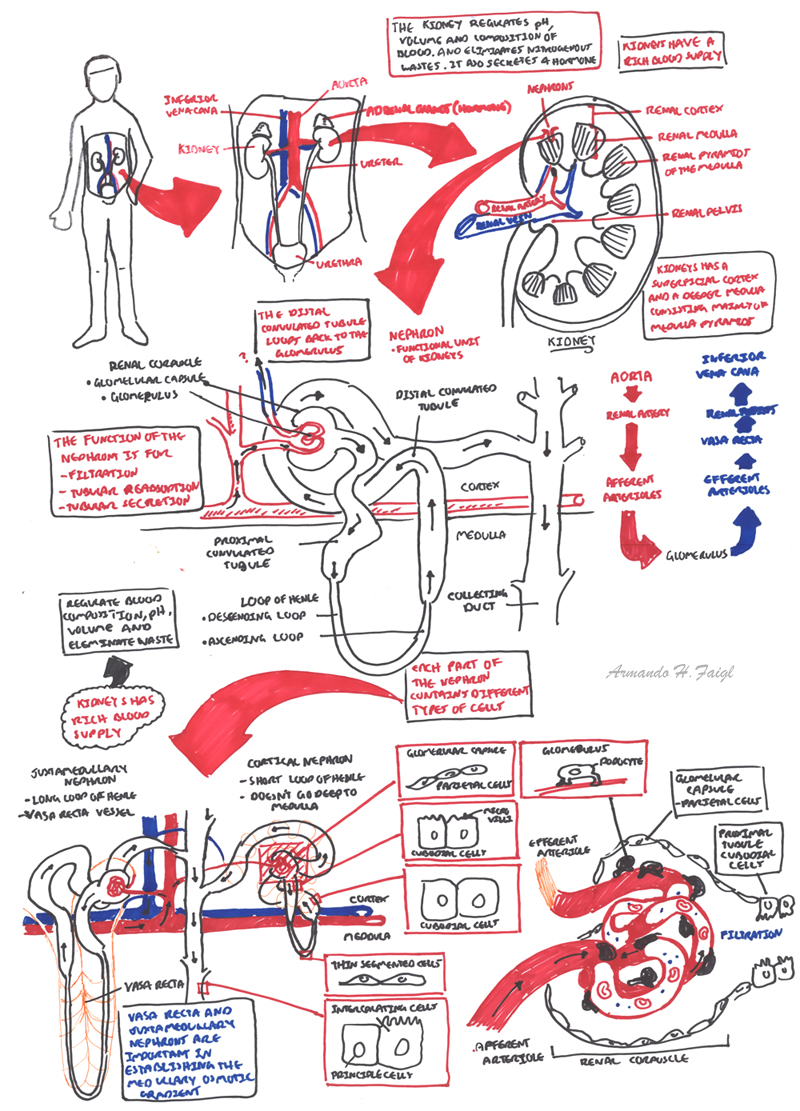
Renal Anatomy
The urinary system consists of:
The kidneys are retroperitoneal bean shaped organs thats sits between veretbral levels T11-L3, the left kidney sitting slightly higher then the right kidney.
The kidneys is divided into three sections:
Arterial Supply
Venous Drainage
Nephrons
Ureters are narrow muscular tube that transport urine to the bladder. There are three narrowed areas of each ureter:
Bladder is a muscular organ which holds urine. The wall of the bladder comprises of four layers:
Urethra Arisis from the base of the bladder and is the passageway through which urine is discharged from the body. The female urethra is much shorter (3-4cm) than the male urethra (18+cm)
| Watch Video Nephrology Overview |
Renal Physiology
| AKI Triad Reduced GFR, reduced urine output and increase in nitrogenous waste in blood. |

| Watch Acute Renal Failure (Injury) |
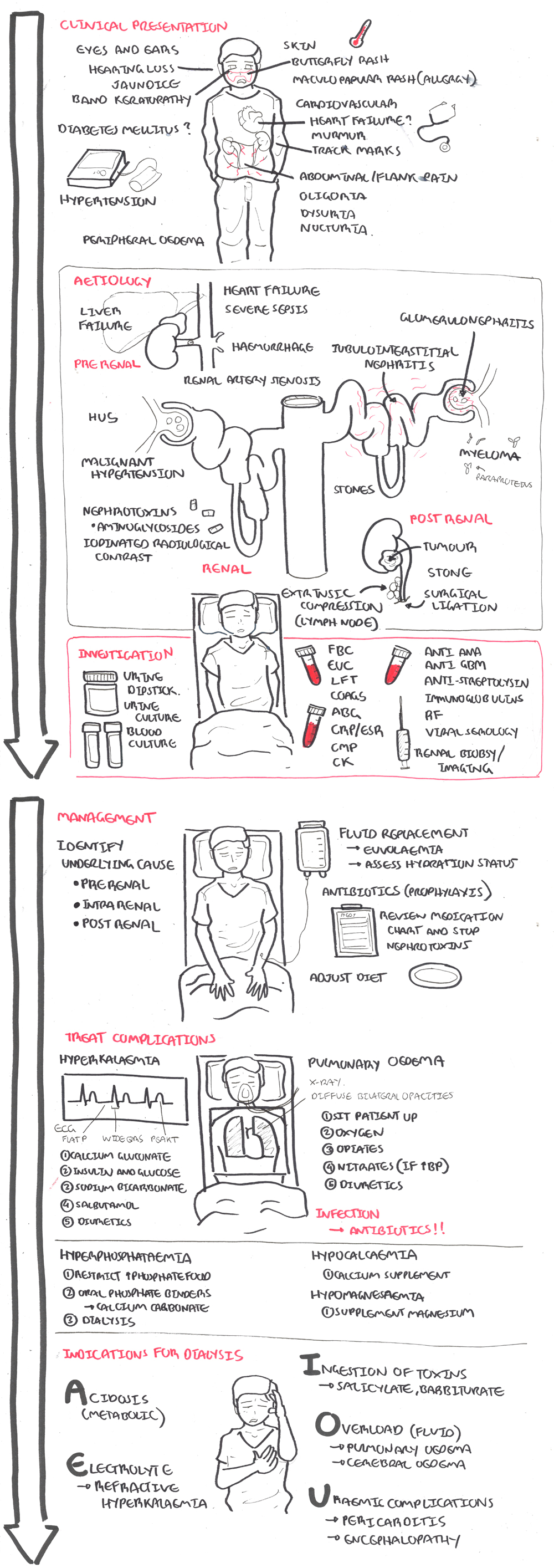
The aetiology of acute kidney injury can be simply divided into pre-renal, renal and post renal causes.
Pre-renal - Sepsis and hypotension:
Intrarenal
Post renal Obstruction:
| Remember Percuss the bladder and perform bladder ultrasound in case the reason for oliguria is bladder in origin. |
Screening for nephritis/nephrotic syndromes
Imaging
Overview Initial treatment should focus on correcting fluid and electrolyte balances and uremia while the cause of acute renal failure is being sought. A volume-depleted patient is resuscitated with saline. The main electrolyte disturbances in the acute setting are hyperkalemia and acidosis.
General
Treat underlying cause
Treat complications
| Remember Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting), flattening of P waves and prolonged PR interval |
| Remember In rhabdomyolysis, Ca2+ can precipitate in injured muscle, causing necrosis and ischaemic contractures—resist the administration of Ca2+ unless symptomatic hypocalcaemia. |
| Side note Sepsis is an important cause of morbidity and mortality in AKI (75% mortality if AKI + sepsis). |
| Indications for Dialysis (AEIOU) |
| Acidosis |
| Electrolytes - refractory hyperkalaemia |
| Ingestions/intoxication - Barbiturates, lithium, alcohol, salicylates, theophyline |
| Overload - Pulmonary oedema |
| Uraemia Complications - pericarditis, refractory pulmonary oedema and encephalopathy |
| Remember Hyperkalaemia can induce cardiac dysrhythmias with the following ECG changes: Peak T waves (tenting) → flattening of P waves and prolonged PR interval |











