Lung Cancer
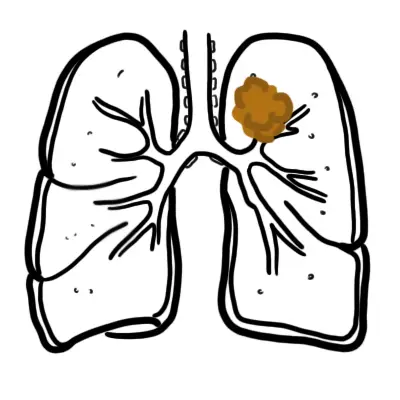

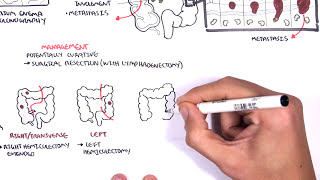
Lung cancer is the leading cause of cancer deaths in men and women. Lung cancer can be divided into small cell and non-small cell carcinoma. Small cell lung carcinoma presents late stage and has poorer prognosis. A solitary pulmonary nodule measuring 8 mm or less can be followed radiographically. For larger lesions, a biopsy, whether bronchoscopic, percutaneous, or surgical, should be considered. Steps in management of a patient with suspected lung cancer include tissue diagnosis, staging, preoperative evaluation, and treatment with surgery, radiotherapy, or chemotherapy.
Massive haemoptysis: More than 500 mL of blood loss that is coughed up within a 24-hour period
Horner Syndrome: Symptoms are ptosis, loss of pupillary dilation (miosis), and loss of sweating on the ipsilateral side (anhidrosis) caused by compression of the superior cervical ganglion and resultant loss of sympathetic innervation.
Superior Vena Cava syndrome: Obstruction of venous drainage, usually by external compression of the SVC, leading to edema of the face, neck, and upper part of the torso often with formation of collateral veins on the upper chest.
There are many risk factors for lung cancer. Smoking, underlying lung disease and exposure to certain chemical are the most common.
Small proportion of patients with lung cancer are asymptomatic when diagnosed. In these cases, a lung nodule usually is found incidentally on chest x-ray or CT. Common signs and symptoms include cough, dyspnea, chest pain, fatigue, weight loss and hemoptysis.
Most patients with hemoptysis require evaluation with bronchoscopy. Massive hemoptysis may result in death by asphyxiation.
General
Investigations for staging
Small cell lung carcinoma (SCLC – 20%)
Non-small cell lung carcinoma ( NSCLC – 80%)
Staging of SCLC is limited or extensive. NSCLC uses the TNM classification for staging.
| Lung cancer characteristics | ||||
| SCLC | Adenocarcinoma | Squamous cell | Large cell | |
| Location | Central | Peripheral | Central | Peripheral |
| Cavitation | Never | Most likely | ||
| Metastases | Early | Early | Late | Late |
| Neoplastic Syndrome and Extrapulmonary manifestation | ADH, ACTH | Thrombophlebitis | PTH | Superior vena cava syndromes + hoarseness |
Once a patient presents with symptoms or radiographic findings suggestive of lung cancer, the next steps are as follows:
Complication
NSCLC
SCLC
Prognosis
Paraneoplastic syndrome are a group of syndromes where cancer cells produce peptides that mimic certain hormones. This occurs through genetic mutations within cancer cells allow them to develop new abilities and become “neuroendocrine cells”. In lung cancer common hormone like substances produced include: PTH, ACTH and ADH.
Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.



















Discussion