Immunoglobulin A vasculitis (IgAV), also known as Henoch–Schönlein purpura, is the most common primary vasculitis in children (peak incidence 4–7 years), with seasonal peaks after upper respiratory tract infections. It is defined as a small-vessel vasculitis with IgA1-dominant immune deposits affecting capillaries, venules, and arterioles, underscoring the central role of IgA in its pathogenesis. Clinically, IgAV can be divided into two forms: a skin-limited form, characterised by cutaneous IgA-dominant vasculitis without systemic organ involvement and manifesting solely as non-thrombocytopenic purpura, and a systemic form, where skin involvement is accompanied by at least one other organ, most commonly the joints, gastrointestinal tract, and kidneys, and rarely the lungs or central nervous system.
The disease is often self-limiting, but recurrence occurs in around one-third of paediatric cases. Renal involvement is the most important determinant of prognosis. Between 20% and 80% of children develop nephritis within four to six weeks of presentation, and 1–7% progress to renal failure or end-stage renal disease (ESRD). IgA vasculitis is milder in children younger than two years, but more severe in adults, with worse outcomes.
Definition
Galactose-deficient IgA1 (Gd-IgA1): Aberrantly O-glycosylated IgA1 subclass prone to forming nephritogenic immune complexes. IgAV nephritis (IgAVN): Kidney involvement in IgA vasculitis, marked by IgA1-dominant immune complex deposition in the glomerular mesangium, leading to haematuria, proteinuria, and variable renal impairment within a systemic small-vessel vasculitis. IgA nephropathy (IgAN): chronic glomerular disease characterised by IgA1-dominant immune complex deposition in the mesangium, causing haematuria, proteinuria, and potential progression to kidney failure. No vasculitis present. Palpable purpura: Non-blanching, raised purpuric lesions from leukocytoclastic vasculitis of dermal venules.
Adults = lower incidence, higher renal risk; always monitor BP, urinalysis, and proteinuria for ≥6–12 months [4,5].
Early proteinuria (>0.5–1 g/day) and hypertension are actionable — start RAAS blockade promptly.
Pathophysiology
IgA vasculitis (IgAV) is a leukocytoclastic vasculitis characterised by IgA-dominant immune complex deposition in small vessels. Two main pathogenic models explain its phenotypes.
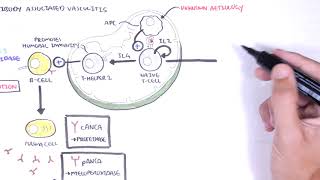
Anti-Gd-IgA1 autoantibodies: IgA vasculitis nephritis (IgAVN) mechanism parallels the “four-hit” theory of IgA nephropathy:
Trigger (often mucosal infection) → overproduction of Gd-IgA1
Formation of anti-Gd-IgA1 autoantibodies → circulating immune complexes
Deposition in small vessels/mesangium → activation of alternative/lectin complement pathways
FcαRI-mediated neutrophil recruitment → leukocytoclastic vasculitis in skin, bowel wall edema/bleeding, mesangial proliferation with proteinuria/hematuria [1,3,11]
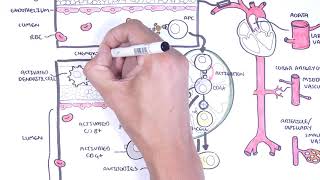
Anti-endothelial cell antibodies (AECA)
Neutrophil-driven small-vessel injury initiated by IgA1-type anti-endothelial cell antibodies (AECA) binding to β2 glycoprotein I receptors on endothelial cells
Induces interleukin-8 production, neutrophil recruitment, and endothelial damage via antibody-dependent cellular cytotoxicity, complement activation, and reactive oxygen species.
Higher serum Gd-IgA1 correlates with extracutaneous/renal involvement in some patients [8,9].
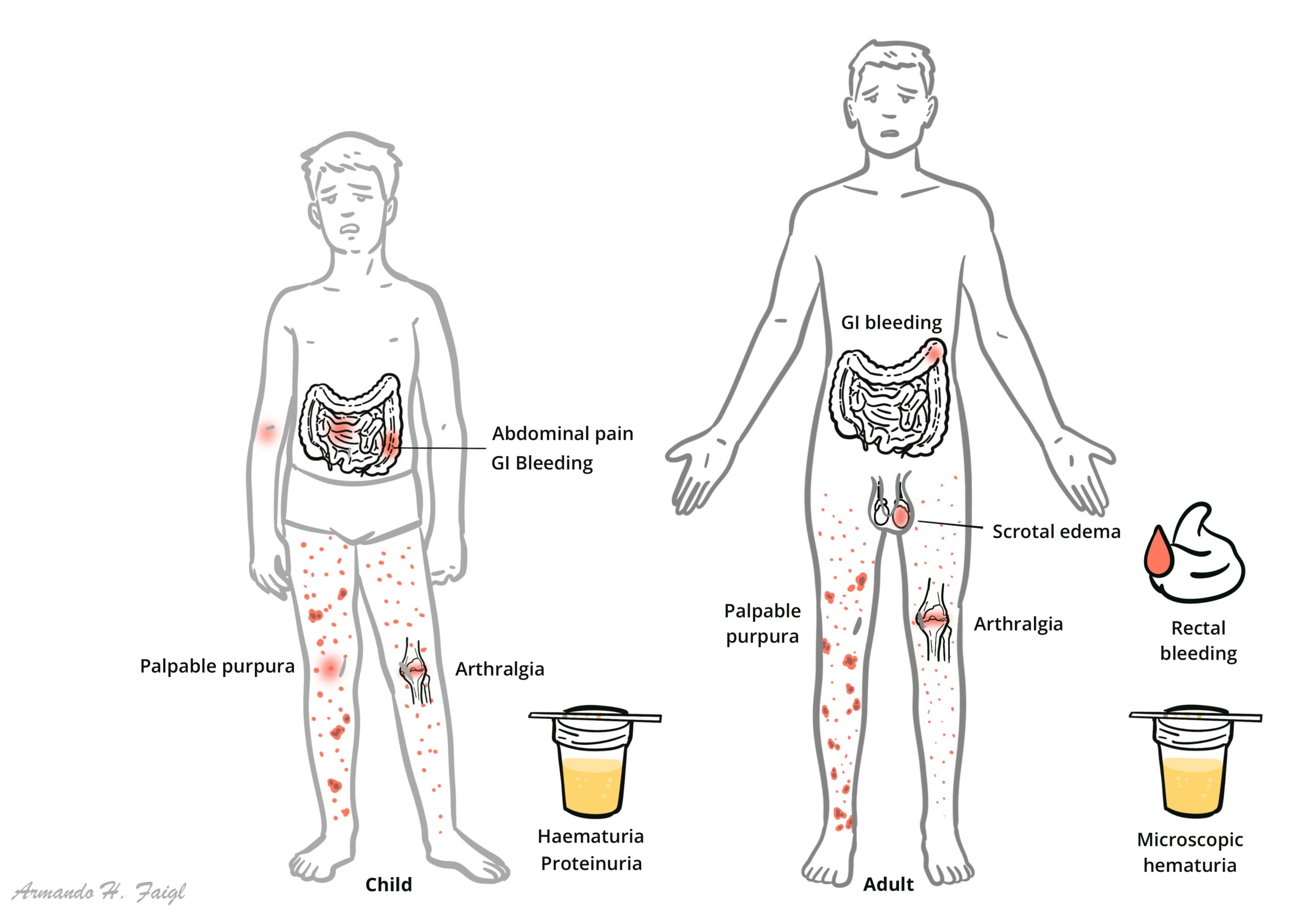
Signs and symptoms may develop over days to weeks in any sequence. The onset of IgA vasculitis typically follows an upper respiratory infection. Joint involvement and abdominal pain are more common in children, whereas adults are more likely to have lower-extremity edema and hypertension.
Cutaneous: Palpable purpura (gravity-dependent; legs/buttocks ± arms/trunk), may form bullae or ulcerate in adults
IgAV spontaneously resolves in >90% of children and 90% of adults, making supportive treatment the primary intervention
IgAV without nephritis is usually self-limiting, especially in children
Higher IgM deposition in skin may indicate potential renal involvement
IgAV with nephritis is associated with worse long-term prognosis. Not self-limiting — chronic inflammation can lead to permanent kidney damage
Prognosis in children generally better than in adults. Adults have more severe and lasting kidney injury.
Children usually recover; adults need long-term renal surveillance.
References
Yang Y, Sun L, Li G, et al. IgA vasculitis update: Epidemiology, pathogenesis, and biomarkers. Front Immunol. 2022;13:921864.
Heineke MH, Ballering AV, Jamin A, Ben Mkaddem S, Monteiro RC, Van Egmond M. New insights in the pathogenesis of immunoglobulin A vasculitis (Henoch–Schönlein purpura). Semin Immunopathol. 2017;39(5):593-607.
Liu LJ, Chen HP, Yu F, Zhao MH. Pathogenesis of IgA Vasculitis: An up-to-date review. Front Immunol. 2021;12:771619.
The Royal Children’s Hospital Melbourne. Clinical Practice Guidelines: Henoch–Schönlein Purpura. 2021 (updated).
KDIGO Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4S):S1-S276.
Hočevar A, Rotar Ž, Jurčić V, et al. IgA vasculitis in adults: performance of the EULAR/PRINTO/PRES classification criteria. Arthritis Res Ther. 2016;18:58.
Bayindir Y, et al. Performance in adults of the EULAR/PReS/Ankara 2008 classification criteria for IgA vasculitis. RMD Open. 2025;11(3):e005728.
Davin JC, Ten Berge IJ, Weening JJ. IgA nephropathy and IgA vasculitis with nephritis share Gd-IgA1-oriented pathogenesis. Kidney Int. 2017;91(3):534-536.
Davin JC, Coppo R. The cause and pathogenesis of IgA nephropathy. Nat Rev Nephrol. 2014;10(6):339-352.
Leone A, et al. Navigating adult-onset IgA vasculitis-associated nephritis. Life (Basel). 2024;14(8):930.
Liu X, et al. Autoantibodies specific for Gd-IgA1 in IgA vasculitis nephritis. Kidney Int Rep. 2019;4(10):1553-1561.
Song Y, et al. Dapsone in refractory IgA vasculitis: systematic review. BMC Nephrol. 2020;21:241.
Kraitsidou E, et al. Adult-onset IgA vasculitis: update on therapy. Rev Med Interne. 2020;41(9):623-630.
Thiel J. What’s new in treatment: IgA vasculitis & IgA nephropathy. The Rheumatologist. 2024.
Glucocorticoids in IgA vasculitis. Acta Medica. 2024;65(4):e1100.

















Discussion