Overview
Acromioclavicular (AC) joint separation is a common shoulder injury, usually sustained from direct trauma such as a fall onto the tip of the shoulder. It involves varying degrees of injury to the stabilising structures of the AC joint — primarily the acromioclavicular and coracoclavicular ligaments. Clinical presentation ranges from localised tenderness and mild pain to obvious deformity with functional limitation, depending on the severity. The Rockwood classification system (Types I–VI) is commonly used to grade these injuries. Most low-grade injuries are managed conservatively with rest, sling support, and physiotherapy, while higher-grade injuries or those causing persistent dysfunction may require surgical stabilisation.
Definition
Acromioclavicular (AC) joint – The articulation between the distal clavicle and acromion of the scapula, important for shoulder girdle stability.
Coracoclavicular (CC) ligaments – The conoid and trapezoid ligaments anchoring the clavicle to the coracoid process, providing vertical stability.
Rockwood classification – A six-type grading system describing the severity of AC joint separation based on ligament disruption and clavicle displacement.
Step-off deformity – A visible or palpable prominence of the distal clavicle relative to the acromion, often seen in higher-grade AC separations.
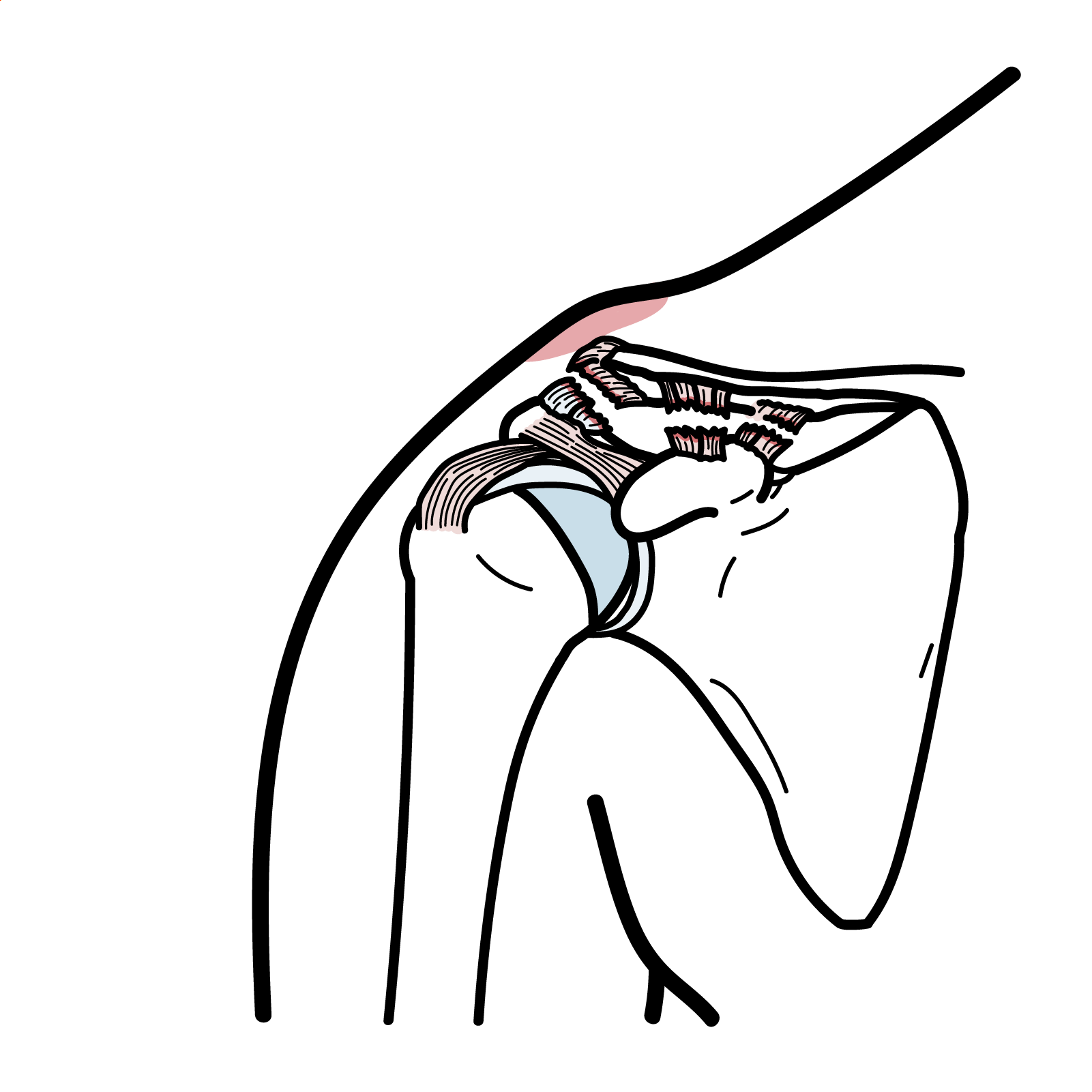
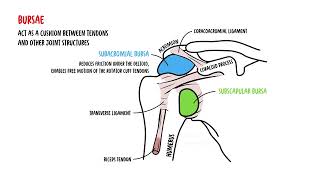
Anatomy & Physiology
- AC joint: Synovial joint between distal clavicle and acromion of scapula
- Stabilizers:
- AC ligaments (anterior, posterior, superior, inferior): Provide horizontal stability.
CC ligaments (conoid and trapezoid): Provide vertical stability.
- Deltoid and trapezius muscles also support the joint
Anatomy & Physiology
- AC joint: Synovial joint between distal clavicle and acromion of scapula.
- Stabilizers:
- AC ligaments (anterior, posterior, superior, inferior): Provide horizontal stability.
CC ligaments (conoid and trapezoid): Provide vertical stability.
- Deltoid and trapezius muscles also support the joint.
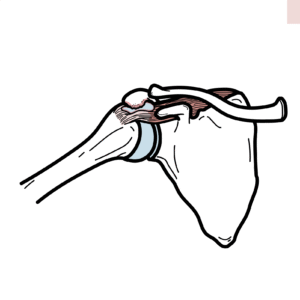
Classification
- Type I: Sprain of AC ligaments only, joint intact.
- Type II: Torn AC ligaments, sprained CC ligaments, mild displacement.
- Type III: Complete disruption of AC and CC ligaments, clavicle displaced upwards.
- Type IV: Posterior displacement of clavicle into trapezius.
- Type V: Severe displacement (>100% increase in CC distance).
- Type VI: Inferior displacement of clavicle under acromion/coracoid (rare).
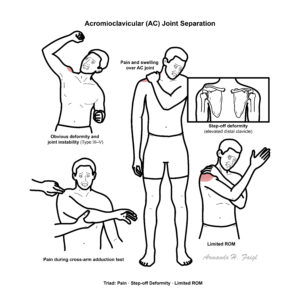
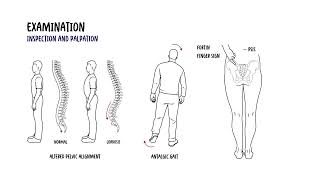
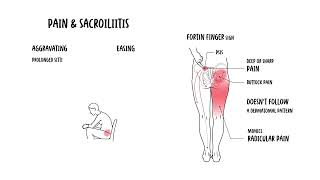
Clinical Manifestations
- Local pain and swelling over AC joint.
- Step-off deformity (prominence of distal clavicle, esp. in type III–V).
- Limited shoulder range of motion due to pain.
- Positive cross-arm adduction test (pain over AC joint).
- In higher grades: obvious deformity and instability.

This image series is only available to members
Triad: Pain, step-off deformity, limited ROM.
Diagnosis
- Clinical diagnosis with history of trauma + localized AC joint pain.
- X-rays:
- AP and Zanca views (10–15° cephalic tilt).
- Compare CC distance with contralateral side.
- Stress views (weights in hands) sometimes used.
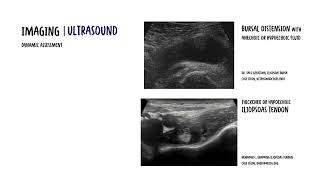
- MRI/Ultrasound: May help in ligamentous injury assessment if diagnosis unclear.
Treatment
- Non-operative (Types I & II, most Type III):
- Sling for comfort (1–2 weeks).
- Ice, NSAIDs, physiotherapy (early range of motion, strengthening).
- Operative (Types IV–VI, selected III):
- Indicated if severe displacement, persistent pain, instability, or high-demand athletes.
- Surgical options: CC ligament reconstruction, hook plate fixation, suture anchors.
Complications & Prognosis
- Complications
- Prognosis
- Most Type I–II injuries: good recovery within weeks.
- Higher-grade injuries: risk of long-term dysfunction if untreated.
References
- Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
- Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, et al. ISAKOS Upper Extremity Committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014 Feb;30(2):271–278.
- Tamaoki MJS, Belloti JC, Lenza M, Matsumoto MH, Gomes Dos Santos JB, Faloppa F. Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst Rev. 2010 Aug 4;(8):CD007429.
- Pallis M, Cameron KL, Svoboda SJ, Owens BD. Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med. 2012 Jan;40(1):207–212.
- Mazzocca AD, Arciero RA, Bicos J. Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med. 2007 Feb;35(2):316–329.
- Taft TN, Wilson FC, Oglesby JW. Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am. 1987 Sep;69(7):1045–1051.












Discussion