

Meniscal Tear

Overview
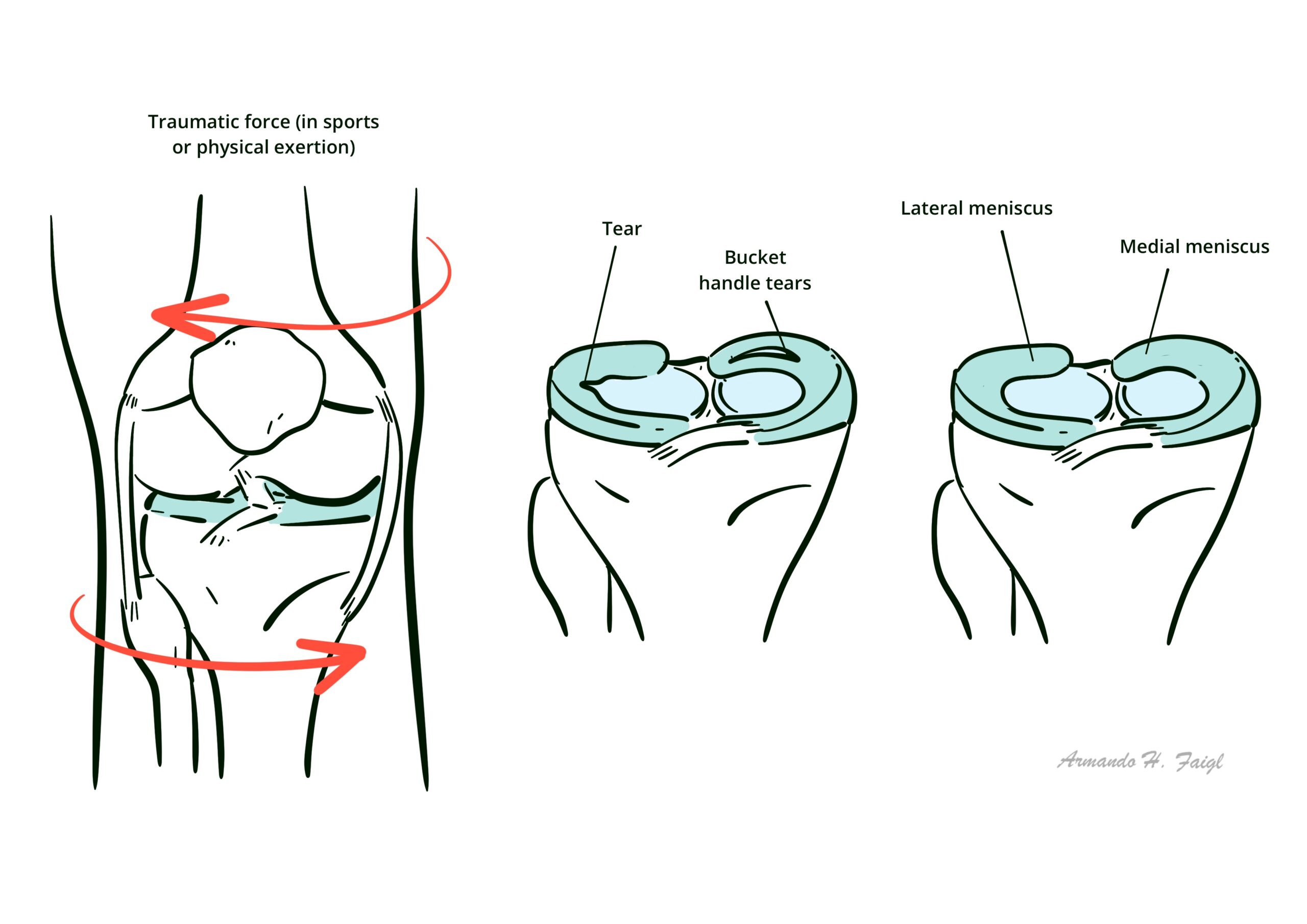
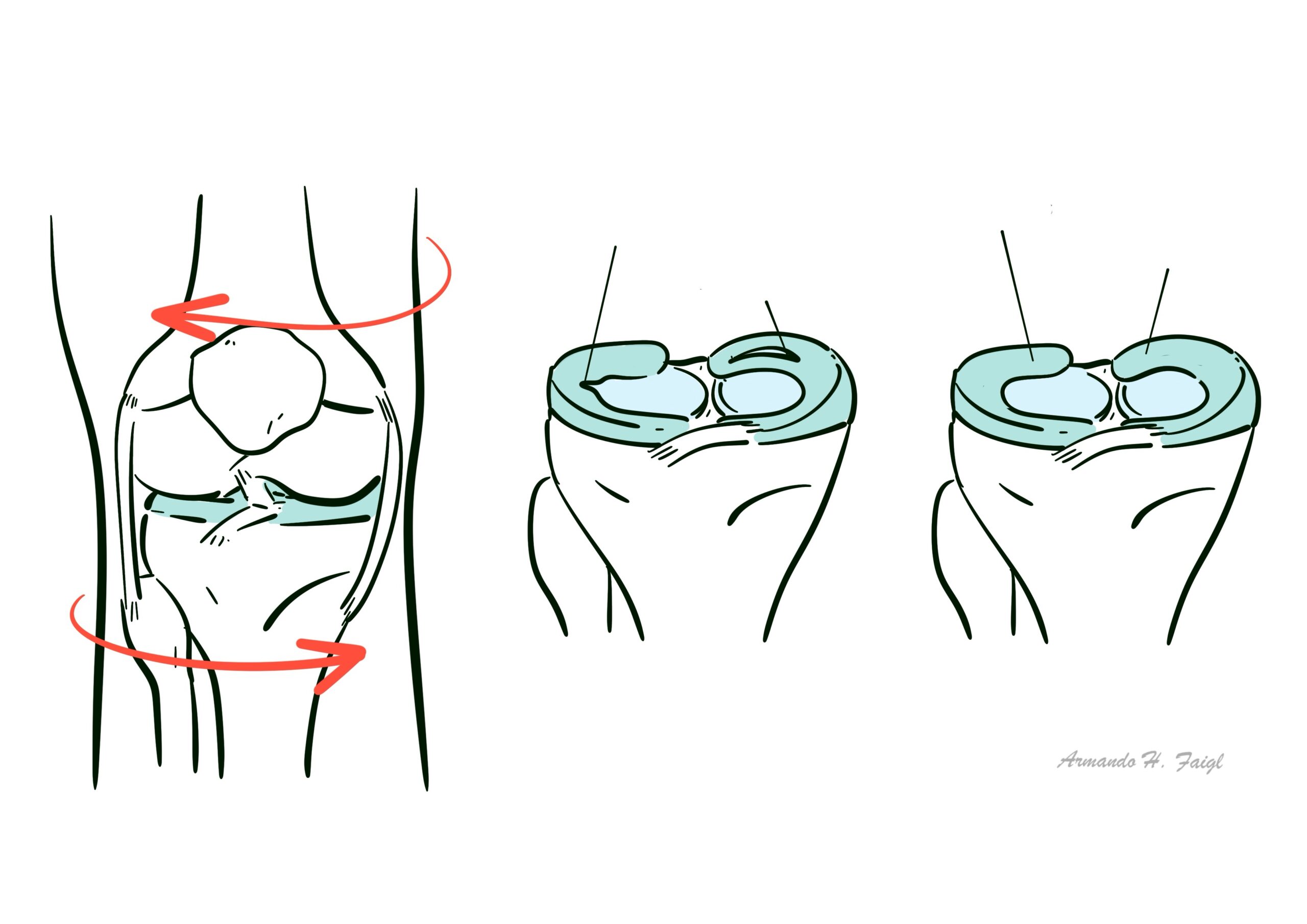
Medial and lateral knee joint menisci serve to transfer load and absorb shock, aid joint stability and provide lubrication. The meniscus is the most commonly injured structure in the knee joint. Acute tears occurs after axial loading combined with rotation. People may complain of a sensation of clicking or catching of the knee with motion. Clinical findigns include positive joint line tenderness, effusion, and positive Mc’Murrary test are important physical exam findings. MRI can help classify location and morphology of meniscal tears.
Definition
Meniscus: The menisci are C-shaped fibrocartilaginous disks in the knee that serve to transfer load and absorb shock, aid joint stability and provide lubrication.
Arthroscopy: is the examination of the inside of a joint, using a special illuminating instrument inserted through a small incision or ‘portal’.
Meniscectomy: is the surgical removal of all or part of a torn meniscus
Anatomy
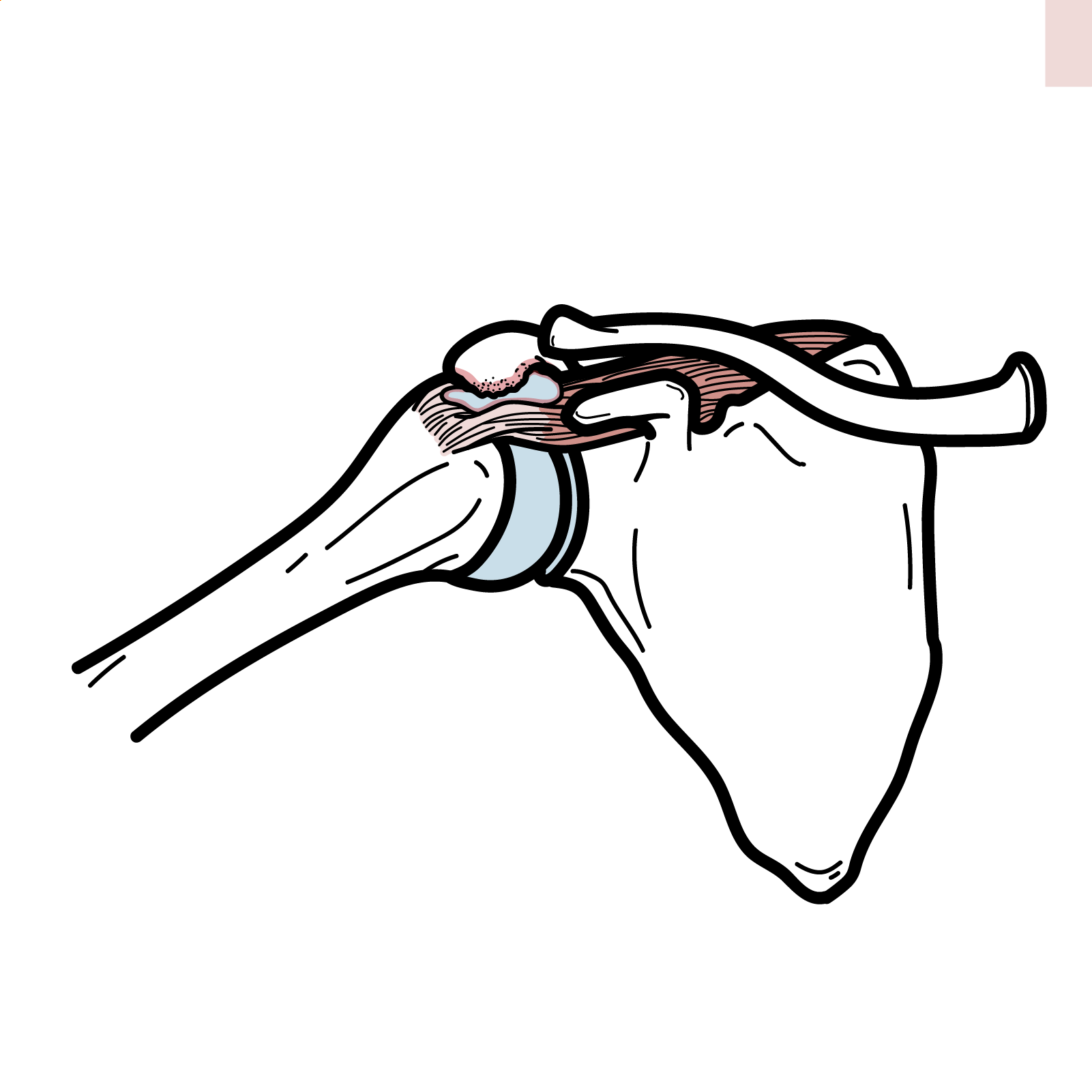
The knee joint is a synovial joint, in that it is encapsulated by the synovial membrane which produced synovial fluid. As the knee is a modified hinge joint it is structured to perform two principal actions, flexion (bending) and extension (straightening). The muscles which act at the knee are predominantly the quadriceps (extension) and the hamstrings (flexion). The knee can also do a bit of internal and external rotation.
The knee joint is made up of three main bones:
- Patella
- Femur
- Tibia.
Cartilage The ends of the bones are covered by articular cartilage. Between these bone articulation there is also the meniscus, another type of cartilage. The menisci are C-shaped fibrocartilaginous disks in the knee (lateral more O-shaped)
The meniscus
Function:
- Provide shock absorption
- Allow for increased congruency between joint surfaces
- Enhance joint stability
- Aid in distribution of synovial fluid
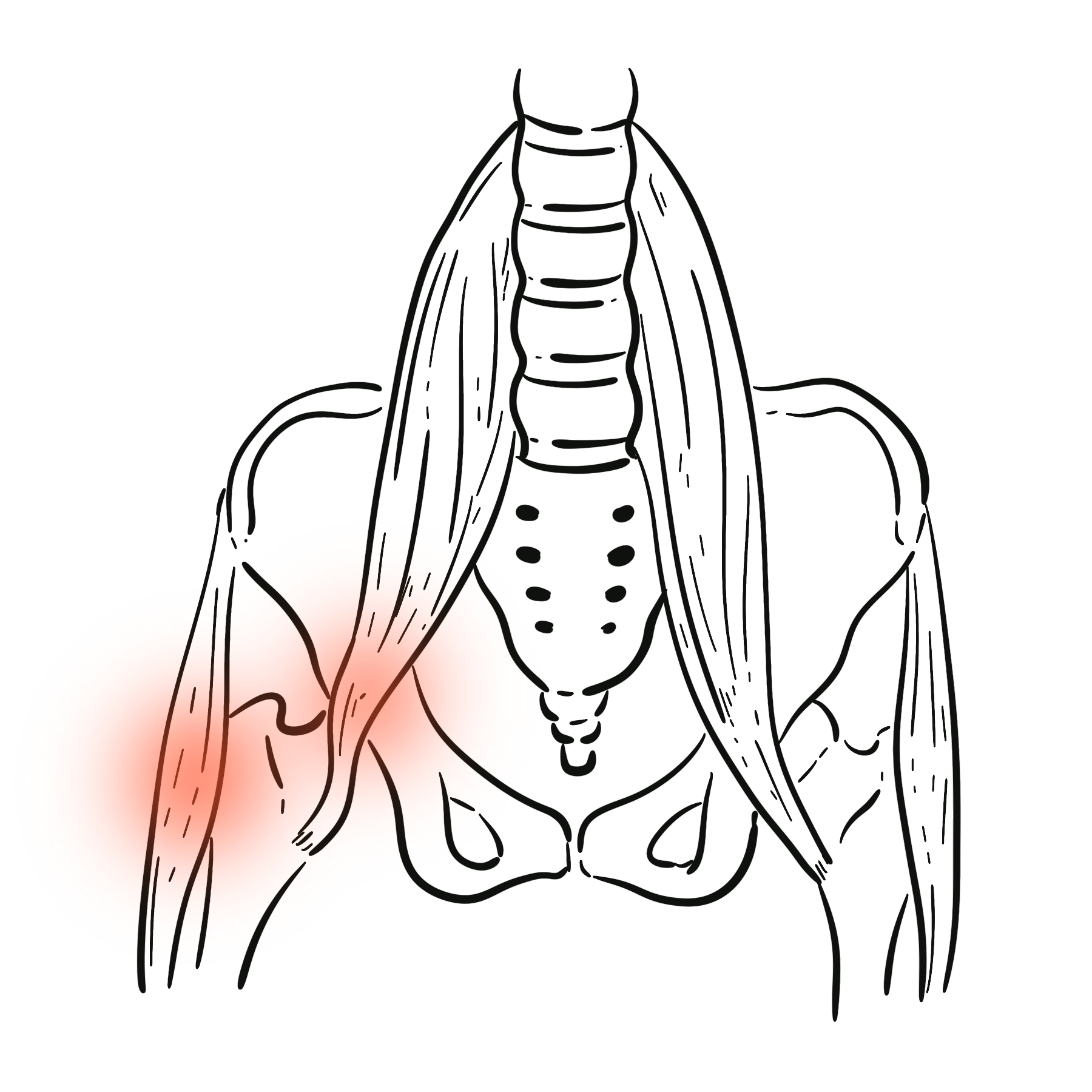
Blood supply The menisci receive blood from branches of the geniculate arteries. The peripheral 1/3 of the meniscus is vascular
The medial meniscus is firmly attached to the joint capsule along its entire peripheral edge. The lateral meniscus there is a region posterolaterally where it is not firmly attached.
The medial meniscus has less mobility than the lateral meniscus and is more susceptible to tearing when trapped between the femoral condyle and tibial plateau.
The lateral meniscus is larger – greater share of the lateral compartment pressure than the medial meniscus carries for the medial compartment.
Atiology & Risk Factors
Aetiology
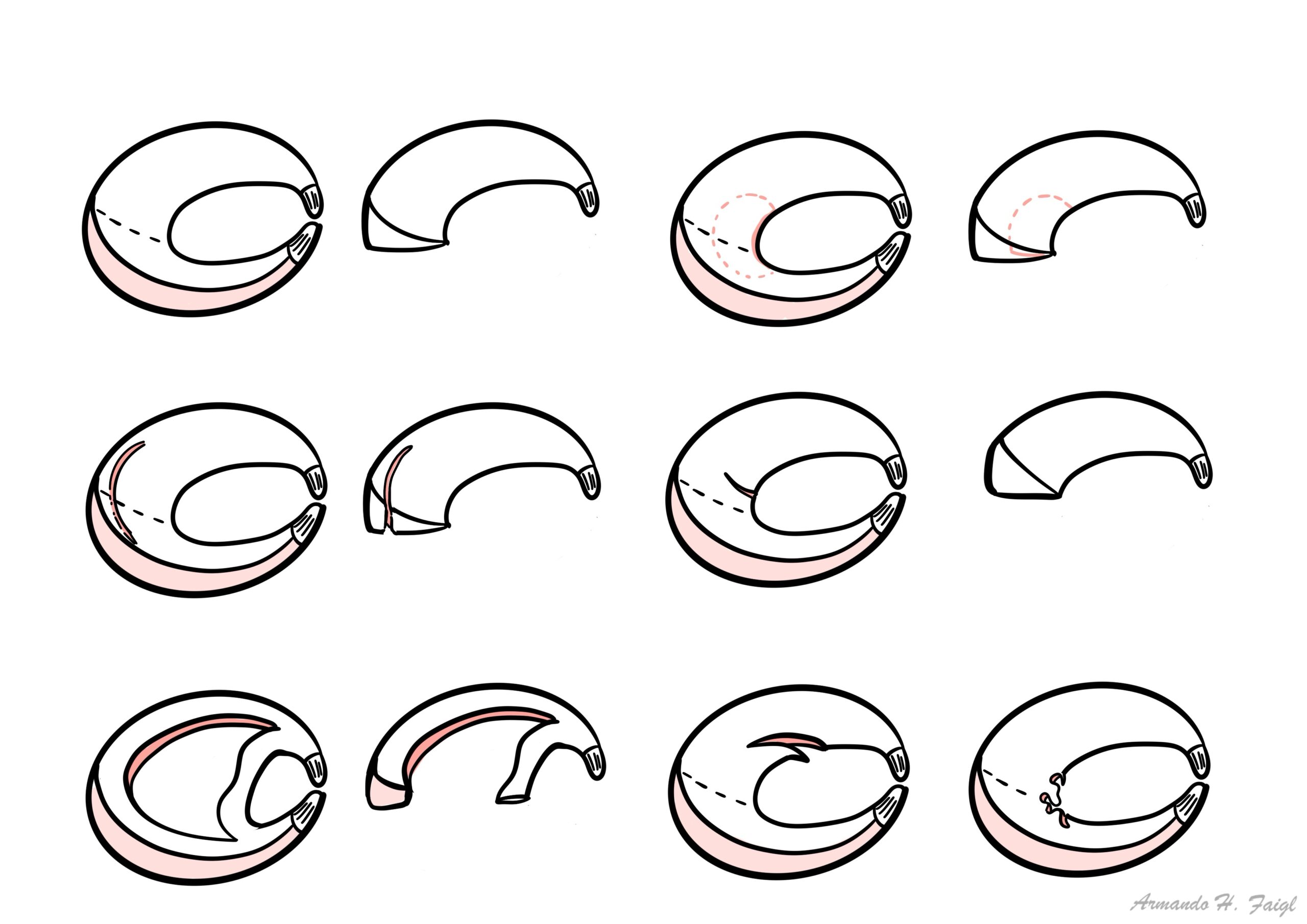
Meniscal tears can be classified either by etiology or by their arthroscopic and MRI appearance.
Etiologic classification divides tears into either acute tears or degenerative tears.
Arthroscopic and MRI appearance:
- Vertical (Longitudinal) Tear → Bucket Handle Tear
- Horizontal Tear → Flap Tear
- Radial Tear→ Parrot-beak
- Degenerative (complex)
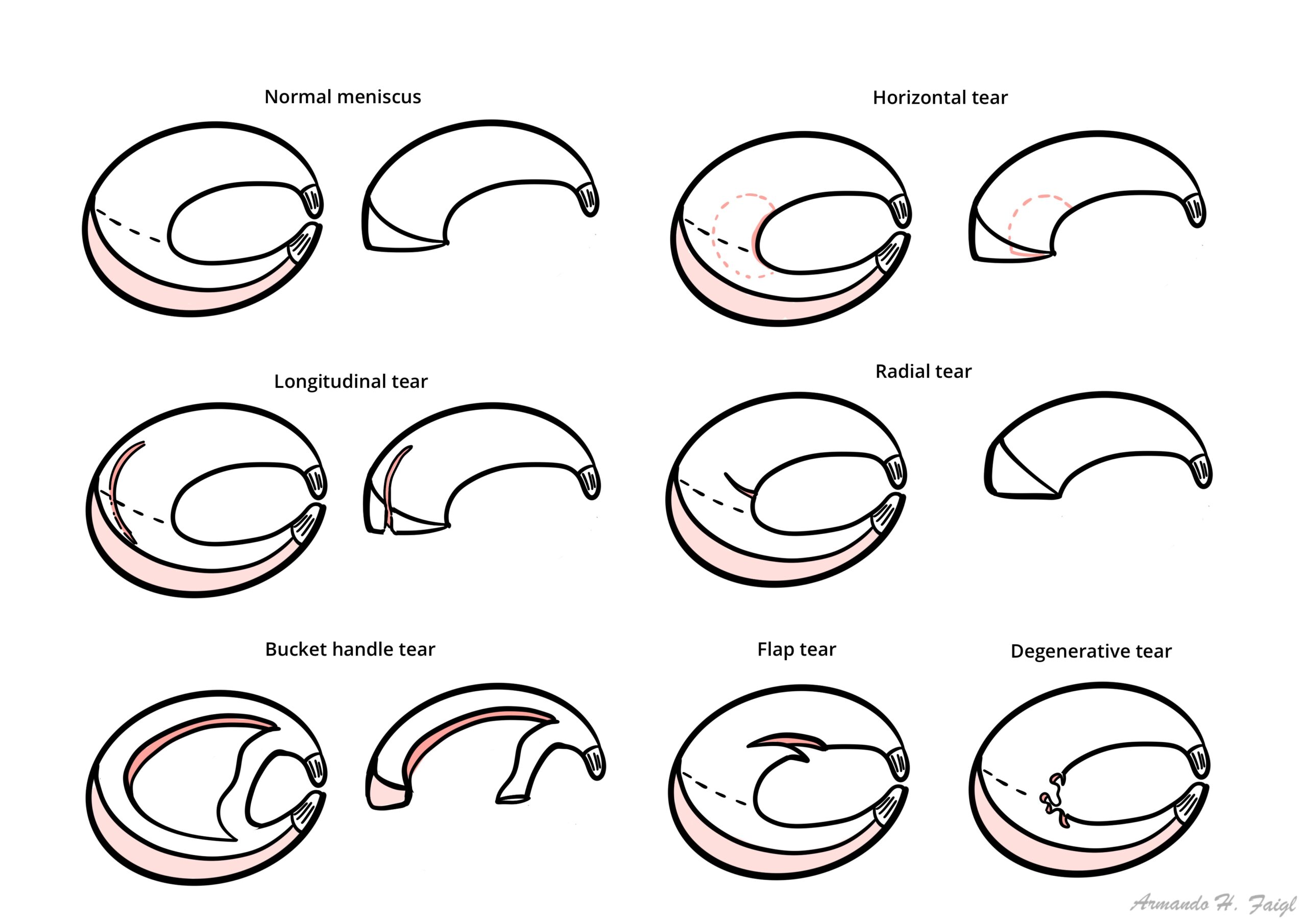
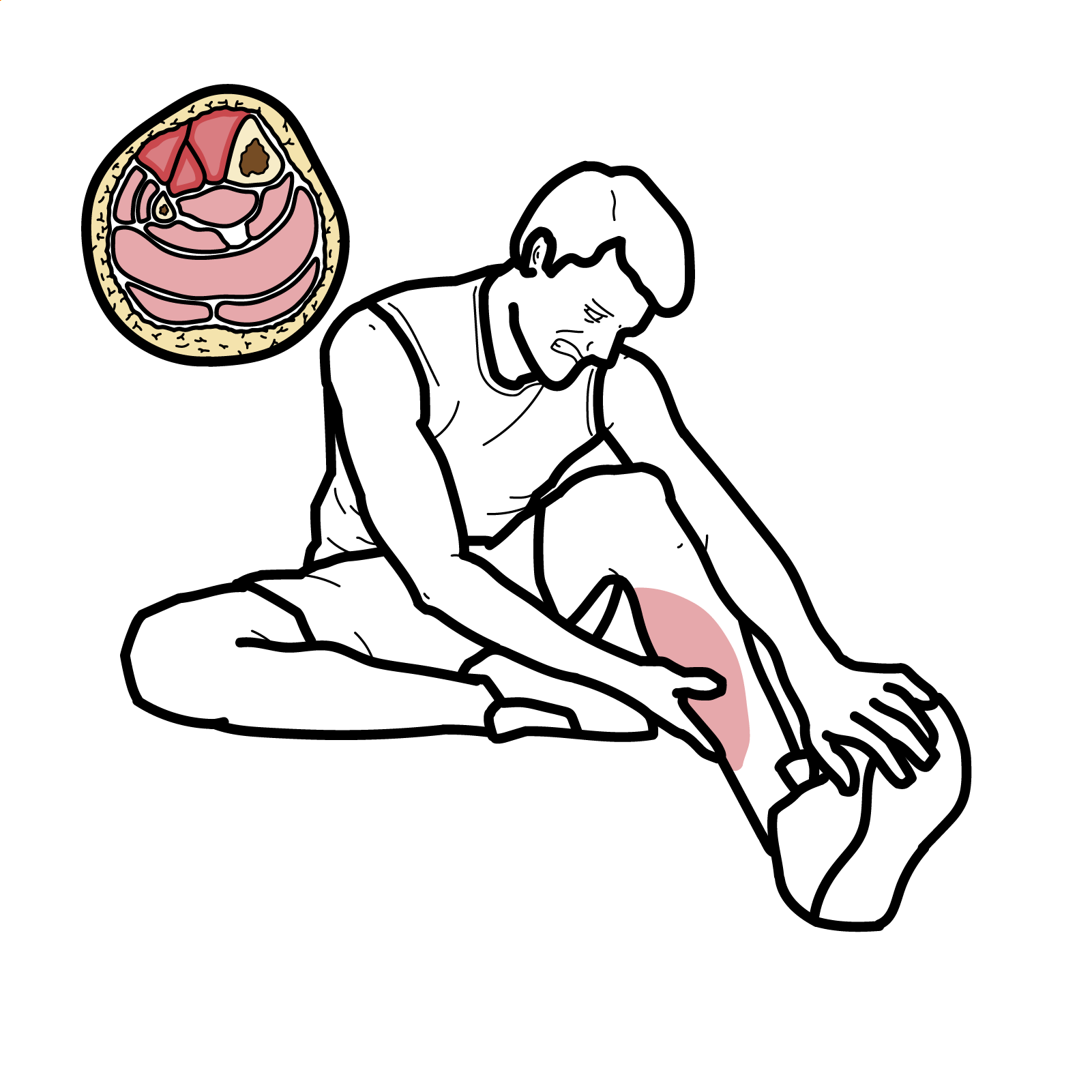
Acute tears For younger patients vertical longitudinal (bucket-handle) are more common. Acute tears occurs after axial loading combined with rotation.
Degenerative tears In older patients, complex and degenerative tears are more common.
- Age
- Sports
- Previous meniscal injury
Clinical Manifestation
Clinical Presentation
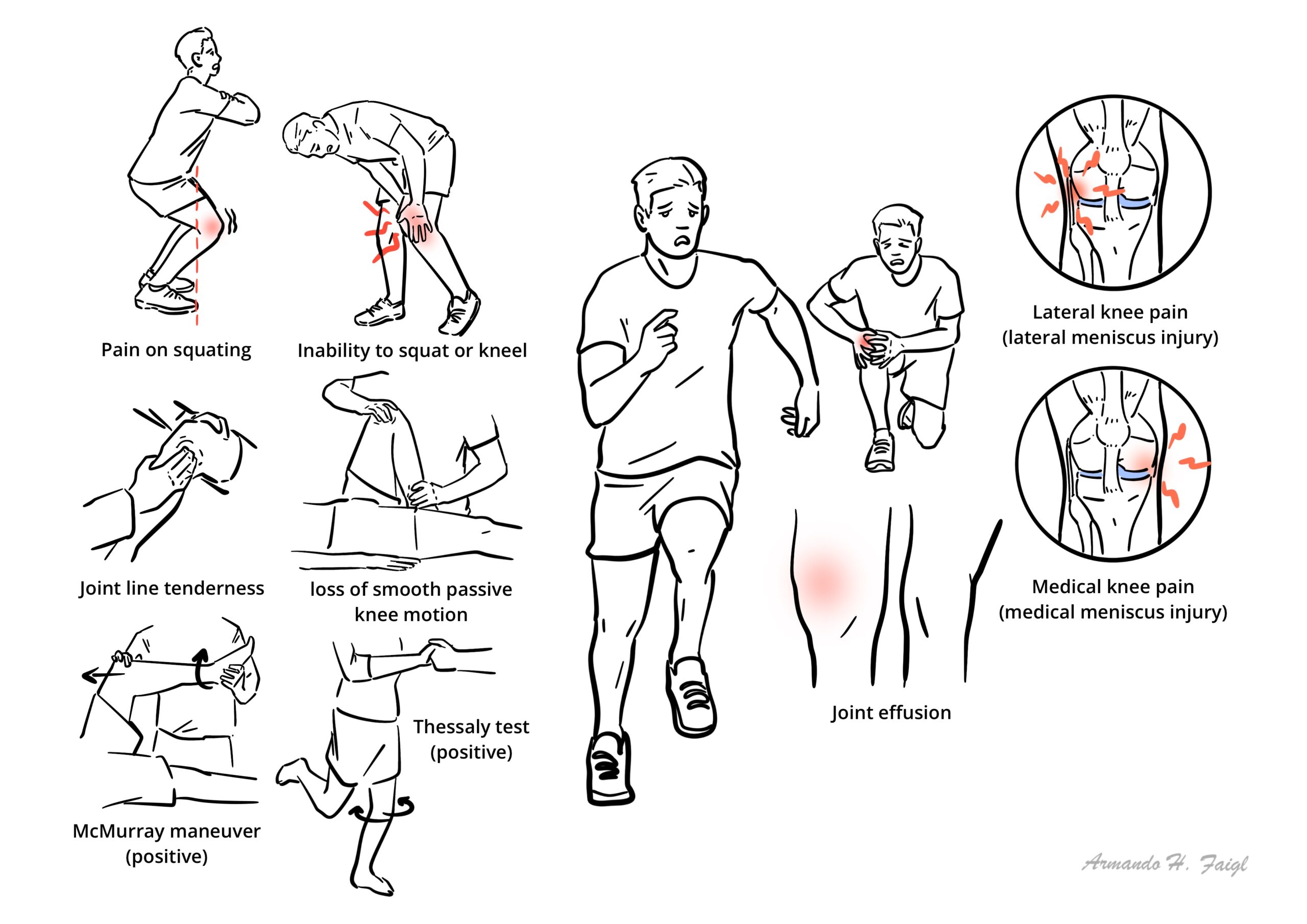
- Medial AND/OR lateral knee pain
- Sensation of catching or locking of the knee joint
- Pain squating
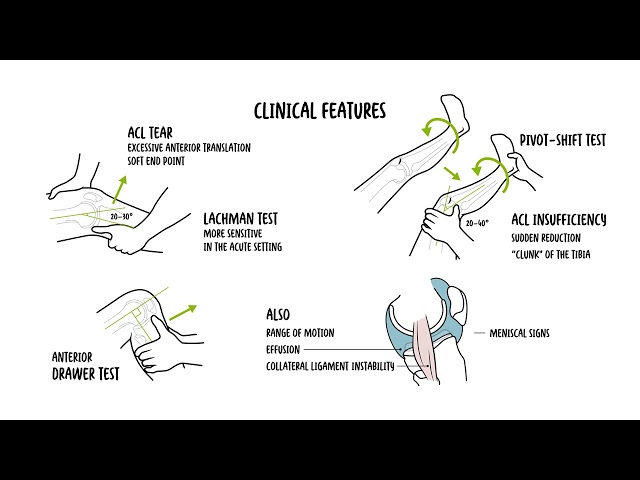
Examination
- Joint line tenderness
- Inability to squat or kneel
- Loss of smooth passive knee motion; inability to extend the knee fully
- Palpable catching on the joint line (McMurray maneuver)
- Pain elicited by specific tests (eg, Thessaly test)
- Joint effusion

The medial meniscus is more frequently torn, partly because of the different shape (less mobility) but also because of its attachment to the medial collateral ligament.
- Meniscal injury – lateral or medial
- ACL tear
- PCL tear
- MCL tear
- PCL tear
- Osteoarthritis (elderly)
O’Donohgue Triad (unhappy triad) Injury to the ACL, MCL and Medial meniscus.
Investigations
- MRI – Magnetic resonance imaging is first line for investigating potential meniscal lesions, but should not replace thorough clinical history and examination.
- X-ray – Plain films of the knee may also show degenerative change, calcification of the meniscus, or calcified loose bodies.
- CT – used if MRI is contraindicated
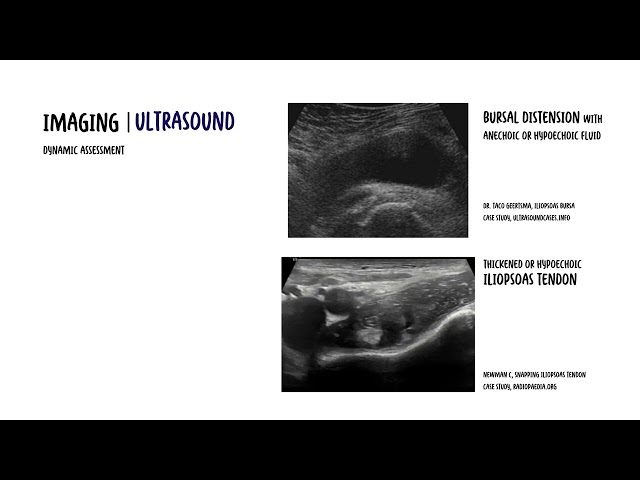
- Ultrasound – increasingly being used? Operator dependent
Treatment
Immediate conservative measures include the RICE regimen:
- Rest (with weight bearing as tolerated or with crutches)
- Ice
- Compression bandaging
- Elevation of the affected limb to minimise acute swelling and inflammation
Small stable meniscus tears often become asymptomatic and do not need to be treated surgically. Those causing persistent symptoms should be assessed with arthroscopy.
Longer term measures include
- Activity modification
- Non-steroidal antinflammatory drugs (NSAIDs)
- Physiotherapy
Pharmacology
NSAIDs inhibit COX1/COX2, enzymes responsible for converting arachadonic acid to Prostagladins, ThromoxaneA2. Prostaglandins promote inflammation, fever and pain. Thromboxane A2 causes platelet aggregation (blood clotting). Side effects: Increased BP, Dyspepsia, Peptic ulcer, duodenal ulcer, liver damage (rare and long-term), acute kidney injury, tinnitus (high-dose) and allergy. Contraindications: Pre-existing renal dysfunction, cardiac failure, severe hepatic dysfunction, history of GI bleeding, allergy, elderly >65.
Surgical Treatment
- Partial Meniscal Resection
- Meniscus repair
- Open
- Arthroscopic
- Meniscal Transplantation
Post surgical rehabilitation is an important part of treatment.
Complications & Prognosis
Complications of surgery including septic arthritis.
References
UpToDate
Oxford Handbook of Clinical Medicine
Best Practice
RACGP Meniscal tear – Presentation, diagnosis and management, 2012





Members only discussions coming soon…