Acute Kidney Injury

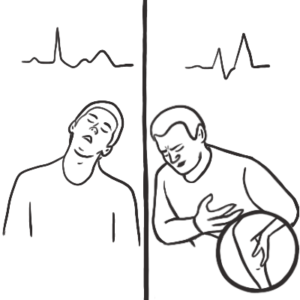
Acute kidney injury (AKI) is the syndrome arising from a rapid fall in GFR (over hours to days). It is characterised by retention of both nitrogenous (including Urea and Creatinine) and non-nitrogenous waste products of metabolism, as well as disordered electrolyte, acid–base, and fluid homeostasis.
| Remember AKI is neither a diagnosis nor a disease. Rather, it is a clinical syndrome that is caused by, or complicates, a wide range of disorders. |
| Definition Acute Kidney Injury: Rapid reduction in kidney function over hours to days, as measured by serum urea and creatinine and leading to a failure to maintain fluid, electrolyte and acid-base homeostasis. Chronic Kidney Disease: Impaired renal function >3months based on abnormal structure or function, or GFR <60 for >3months. Oliguria: A urine output of <400ml/day may be the earlier sign of impaired renal function. |
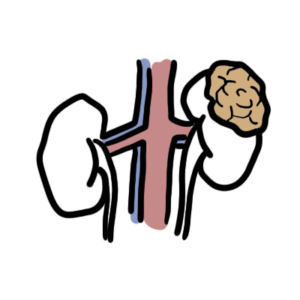
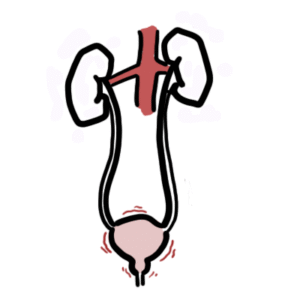
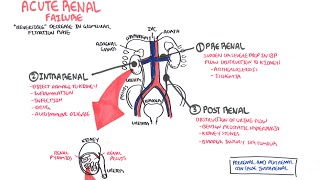
The aetiology of acute kidney injury can be simply divided into pre-renal, renal and post renal causes.
History
Examination
Bedside test
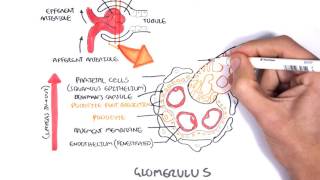
Drawing for urine sediment examination….













Discussion