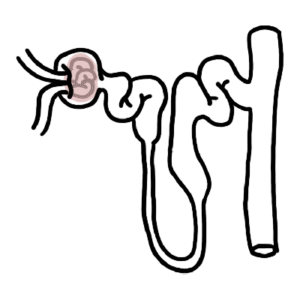
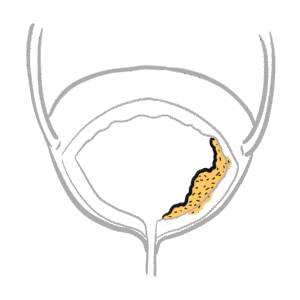
0:00 Renal tract stones are kidney stones, also known as urolithiasis, are common, 0:17 affecting 0:18 roughly 2-3% of people in western countries. 0:21 They're more frequent men and typically occur in people under 65. 0:26 They usually form in the kidney first, and if they move into the drainage 0:30 system, they 0:30 can become uroteric stones, which is when they often cause symptoms. 0:37 Now, there are many types of kidney stones, about 80% of urinary tract stones 0:45 are calcium-based. 0:48 These include calcium oxalate, calcium, phosphate, and mixed stones. 0:53 The remaining types include stuvite stones, which are also known as infection 0:57 stones from 0:58 chronic urinary tract infections. 1:01 Urate stones, notably because they are typically radiolucine on plain x-ray and 1:06 they are associated 1:07 with high uric acid levels. 1:10 And finally, cysteine stones, which are very uncommon and often linked to 1:14 inherited metabolic 1:16 disorders. 1:18 Stavine stones can actually grow quite large and may form staghorn caculi, 1:23 where the stone 1:24 fills much of the renal pelvis, as shown here. 1:28 So, why do stones form? 1:32 Well, stones form when urine becomes oversaturated, put it simply, meaning 1:40 mineral concentrations 1:43 are high enough that crystals precipitate. 1:48 So calcium and oxalate precipitate relatively easily, which is why calcium 1:53 stones are most 1:54 common. 1:57 Some stone types point to specific drivers. 2:00 For example, stuvite stones form an alkaline urine, with urease-producing 2:05 organisms such 2:06 as protis or klebsiella. 2:10 Stuvite stones are associated with increased urate production, often from diet, 2:15 or conditions 2:15 like myeloproliferative disorders. 2:19 Cysteine stones occur with inherited disorders affecting cysteine handling, 2:24 leading to recurrent 2:25 stone formation. 2:31 Some clinical anatomy, there are some specific sites where ureteric stones get 2:37 stuck. 2:37 When a stone enters the ureter, which is the tube connecting the kidney to the 2:42 bladder, 2:42 it commonly lodges at three natural, narrow points. 2:47 These are your pelvic ureteric junction, the crossing of the pelvic brim near 2:52 the ileic 2:53 vessel, and the vesico ureteric junction. 3:02 The classic presentation of a kidney stone, or a renal ureteric colic, is 3:10 people get a 3:11 sudden, severe pain that radiates from the flank towards the groin, loin to 3:18 groin, often 3:19 with nausea and vomiting. 3:21 Distal ureteric stones may cause urinary frequency or urgency. 3:27 D-maturia is very common, often microscopic, rather than visible. 3:32 If infection is present, patients may develop fevers, rheagors, lethargy, and 3:36 in severe 3:36 cases sepsis. 3:39 Examination may show flank tenonus and dehydration, although it can otherwise 3:45 be unremarkable. 3:46 Some stones can be painless, especially if non-obstructing. 3:55 There are important differentials for flank pain in someone less than 65, 4:00 especially, 4:02 so you've got to think about pylonephritis, ruptured abdominal aortic aneurysm 4:06 is very 4:07 serious, ability pathology, bowel obstruction, lower lob pneumonia, and vascul 4:13 oskeletal pain. 4:20 So if someone presents with a suspicion of a renal stone, a urine dipstick may 4:26 show microscopic 4:27 hematuria and also signs of infection. 4:31 Of course, if infection is suspected, send a urine culture, as well as a blood 4:36 culture. 4:37 Blood tests typically include full blood count and CRP to look for inflammation 4:41 or infection, 4:42 and urea electrolytes for renal function. 4:46 Serum calcium and urate can help, and if the patient passes a stone, sending it 4:51 for stone 4:53 analysis is valuable, because you can check that particular stone, what it is 4:59 made of, 4:59 is it calcium oxalate, calcium phosphate, spruvite, etc. 5:09 In terms of imaging, the diagnostic gold standard for a renal stone is a non- 5:14 contrast CTKUB, 5:17 which has high sensitivity specificity and can it detect alternate pathologies. 5:22 This image, for example, demonstrates a 4mm Calculi in the right ureter at the 5:28 level of 5:29 L3 for disc. 5:31 It is associated with mild hydro nephrosis, an extensive periureterican peri 5:38 renal stranding, 5:41 so there's a lot of irritation of the ureter and the kidneys due to this 5:46 particularly small 5:47 stone. 5:52 Ultrasound can assess for hydro nephrosis and may detect renal stones, but 5:57 often misses 5:58 ureteric stones, with the advantage of no radiation. 6:02 Here a ureteric stone causing right, moderate, hydro, uretero nephrosis. 6:10 You can see the ureter is big on the left side here, which is actually the 6:18 right ureter. 6:20 Plain abdominal x-ray isn't usually first-line, but may be used for 6:24 surveillance of known 6:25 radio opaque stones. 6:28 Here you can see an x-ray of an enlarged left kidney. 6:32 There are a large number of huge stones in the left kidney, a combination of 6:36 central 6:36 collection system, centered stone and cortical stones. 6:41 There is no ureteric stones in this x-ray, there is otherwise you can't see 6:45 hydro nephrosis. 6:55 In terms of management, someone comes in with a kidney stone. 7:00 Many patients are often dehydrated, especially vomiting, so provide fluids as 7:05 needed initially. 7:07 Analgesia is key and anti-inflammatories, including perurrectum are often very 7:11 effective. 7:12 Most stones pass spontaneously, particularly if the stones are distal stones or 7:19 less than 7:20 5 millimeters in diameter. 7:24 Any concern for infection or sepsis warrants IV antibiotics and urgent urology 7:30 review. 7:31 Admission is often needed for post-abstructive acute kidney injury, 7:35 uncontrolled pain-infected 7:37 stones or large stones unlikely to pass. 7:45 Of course, if a stone is obstructing the actual flow of urine, you need decomp 7:53 ression. 7:55 So if an obstructing stone especially is associated with infection or renal 8:00 impairment, urgent 8:01 decompression is required. 8:04 And this can be done with a ureteric stent placed retrograde via systoscopy or 8:10 a nephrostomy 8:12 placed directly into the renal pelvis to drain urine above the obstruction. 8:23 Once the initial management is done, whether the stone passes or it doesn't and 8:30 it just 8:30 doesn't cause pain, you still have to treat the actual cause. 8:37 So there is a definitive stone treatment, definitive options include ESWL or 8:43 shockwave 8:44 lithotripsy for small stones often less than 2 centimeters, it's not suitable 8:49 in pregnancy 8:49 or significant bleeding risk or using anticoagulation. 8:55 The other option is ureteroscopy with laser lithotripsy and fragment removal, 9:00 especially 9:01 for ureteric stones. 9:03 Accutaneous nephro lithotomy for large renal stones including stag horn calculi 9:15 . 9:16 Key complications for urolytheosis or kidney stones are really infections and 9:21 post-renal 9:22 acute kidney injury. 9:25 Because obviously when you obstruct the flow of urine in the ureter, the urine 9:31 goes backwards 9:33 essentially causing kidney damage. 9:37 Both infection and post-renal acute kidney injury are treatable if managed 9:43 early. 9:44 Recurrent stones can cause scarring and contribute to chronic loss of renal 9:52 function. 9:53 All recurrent stone formers should be advised to stay well hydrated and have 9:58 serum calcium 9:59 and urate checked if stone analysis isn't available. 10:03 Prevention depends on stone type, dietary oxalate advice for oxalate stones, 10:08 reducing 10:08 salt and checking PTH for calcium stone formers, dietary purine reduction, 10:14 possible urate 10:15 lowering therapy for urate stone and consideration of inherited cause for cyste 10:22 ine stones. 10:23 Now, just a quick touch on bladder stones. 10:29 Bladder stones usually form due to urinary stasis, commonly from chronic 10:34 retention and 10:35 presents with lower urinary tract symptoms. 10:38 They're typically managed via systoscopy and fragmentation if needed, and 10:42 underlying 10:43 bladder outlet obstruction should be considered especially in men. 10:47 Like irritation from bladder stones may increase long-term bladder risk. 10:58 So in summary, we talked about urolithiasis, which is essentially stone 11:02 formation in the 11:03 urinary tract. 11:05 We really talked about how stone is formed in the kidneys from over saturation 11:11 of urine 11:11 and how it can move down the ureter, and there are three common sites where the 11:16 ureter 11:17 risk stones get stuck, and we learned about the typical features loin to groin 11:23 nausea 11:23 vomiting. 11:24 Thank you for watching.