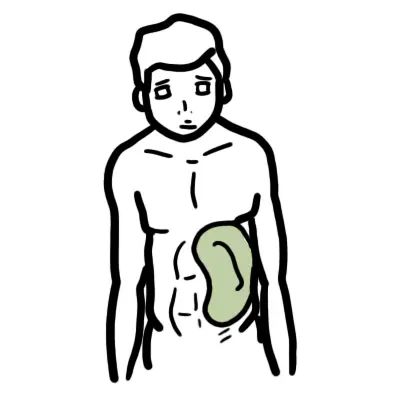
Splenomegaly generally denotes a palpably enlarged spleen. Splenomegaly can be found in 3% of the normal population. Causes of an enlarged spleen are multiple (hepatic, haemotological, infection or inflammation).
Definition
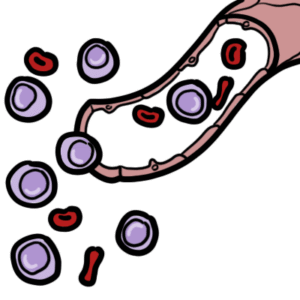
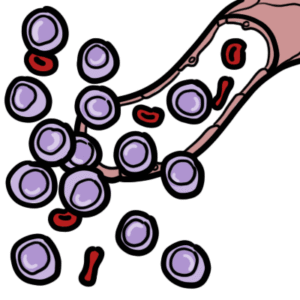
Hypersplenomegaly: abnormal enlargement of the spleen Hypersplenism: defined as one or more blood cytopenias in the setting of splenomegaly. Pancytopaenia: reduction in the number of RBCs, WBCs, and platelets in the peripheral blood below the lower limits of the age-adjusted normal range for healthy people. It is therefore the combination of anaemia, leukopenia, and thrombocytopenia.
Anatomy of the Spleen
Location: Left hypochondrium
Rule of odds (1,3,5,7,9-11):
1 inch thick
3 inches broad
5 inches long
7 ounces weight
Underlies 9-11 ribs
Position: obliquely along long axis of 10th rib; directed downward, forward and laterally
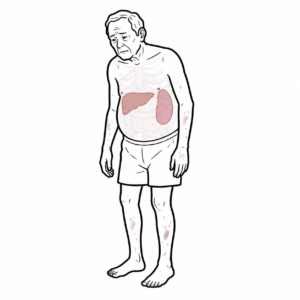
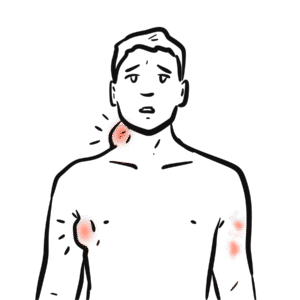
Petechiae and ecchymoses – thrombocytopaenia , malignant haemotolgic disease
Proper examination of the spleen requires relaxation of both the abdominal musculature (arms at the side of abdomen) of the patient and the examiner hands (beware of tender spleen).
Difference Between Enlarged Spleen and Kidney Examination
Rashes and or joint swelling – Systemic autoimmune disease
Petechiae and ecchymoses – thrombocytopaenia , malignant haemotologic disease
Spider angiomata or spider naevus are common on the face and upper chest. They are given that name because they have a central red papule with feeding capillary legs. Occur in presence of extra oestrogen (pregnancy or liver disease).
Splenectomy is surgery to remove the entire spleen
Problems after splenectomy:
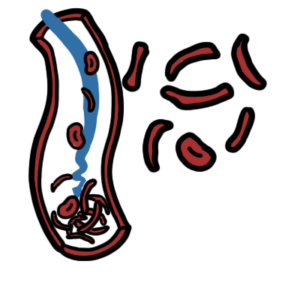
Immediate: Increased platelet count may lead to thromboembolic phenomenon
Long-term: Increased risk of infection with capsulated organisms (like Streptococcus pneumoniae, Nisseria meningitidis, H.influenzae or E.coli), malarial parasites, babesia
Prophylaxis for Post-splenectomy infection:
Vaccinate 2-3 weeks before elective splenectomy: Pneumococcal vaccine, Hemophilus influenza type B (Hib) vaccine, Meningococcal group C vaccine, Influenza vaccine
Lifelong Antibiotic prophylaxis: Long-term penicillin V 500mg 12 hourly (erythromycin if allergic to penicillin)
Revaccination of pneumococcal vaccine: in every 5 years and influenza vaccine anually
Antimalarial chemoprophylaxis: if needed (travel to endemic area)
Post splenectomy hematological features:
Thrombocytosis: persists in 30% cases
WBC count: usually normal but there may be mild lymphocytosis and monocytosis













Discussion