Asthma in Emergency
Introduction
Most asthma deaths occur outside hospital and are:
- In patients with chronic severe disease
- In those receiving inadequate medical treatment
- In those who have been symptomatically deteriorating, and may have already sought medical help
- Associated with adverse behavioural and psychological factors
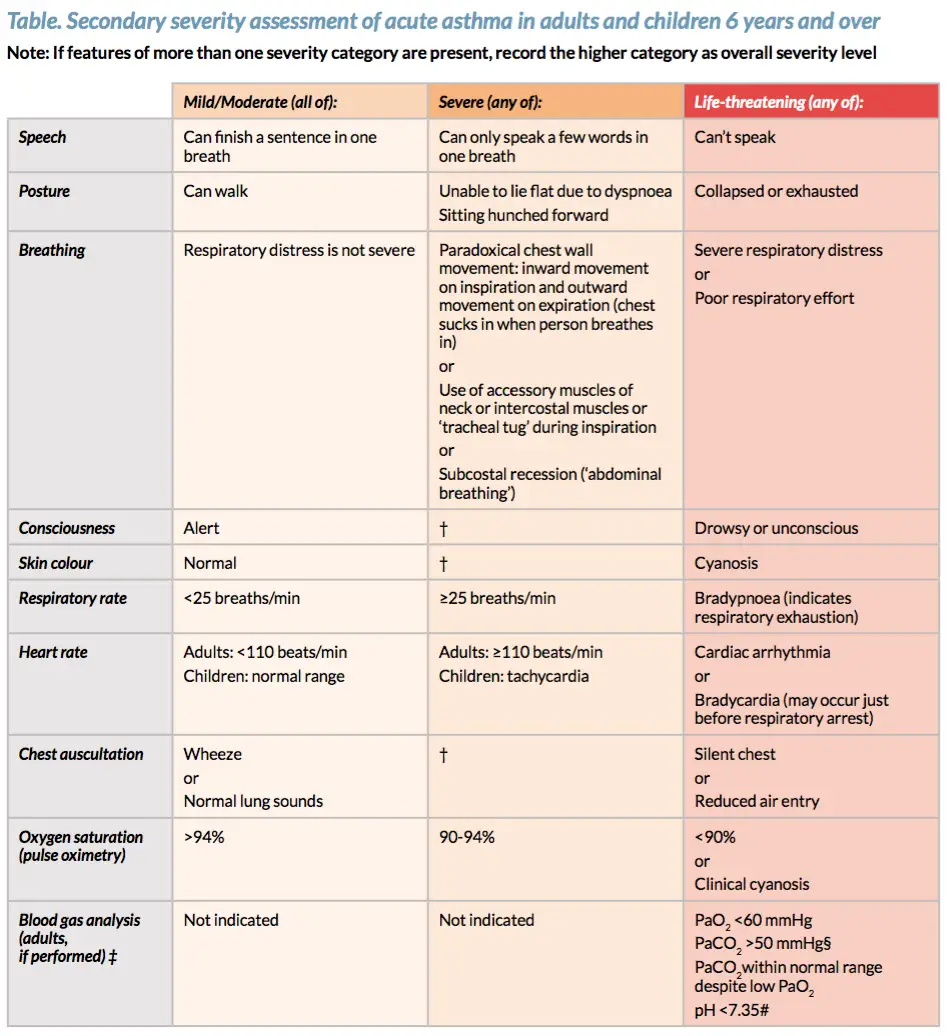
Asthma Assessment
Assess severity and start bronchodilators!
Mild-Moderate (maybe admitted to hospital or more likely may improve and go home)
- SaO2 >95% room air
- Tachypnea <25
- Able to talk in sentences or phrases
- No accessory muscle use
- Alert
- Skin colour: Normal
- Chest auscultation: Normal or Wheeze
Severe (admitted to hospital)
- SaO2 90- 95% room air
- Tachypnea >25bmp
- Mild to moderate tachycardia for age
- Can only speak a few words in one breath
- Mild-moderate use of accessory muscle
- Skin colour: Pallor
- Chest auscultation: Wheeze
Life-Threatening (Admitted to hospital possible transferred to a higher level faculty)
- SaO2 <90% room air
- Tachypnea >30
- Tachycardia or Bradycardia
- Able to talk in words or unable to speak or cry
- Moderate to severe accessory muscle use
- Agitation, drowsy or confused
- Skin colour: Cyanosis
- Chest auscultation: Silent chest or reduced air entry
Take note if person can talk in whole sentences, phrases, words or can’t talk at all!
Mild/Moderate Asthma
Assess severity and start bronchodilators!
Mild (maybe admitted to hospital or more likely may improve and go home)
- SaO2 >95% room air
- Able to talk in sentences
- No accessory muscle use
- Alert
Treatment
- Short-acting Beta2 receptor agonist (ie. Salbutamol with spacer)
- Reassess, Repeat bronchodilator, Reassess, Repeat
- +/- Anticholinergic – Ipratobium bromide (if bronchodilator alone has poor response)
- Reassess, Repeat Ipatropium bromide, Reassess, Repeat
- Oral prednisolone
- Reassess at 1 hour after starting bronchodilator, monitor and continue discharge
- Continue to severe management if not improving
If not responding to any treatment during the 1 hour after bronchodilator, immediate transfer to high level care → move to life-threatening management.
Discharge
- Discharge summary
- Discharge medication (+spacer)
- Educate
- Asthma action plan
- Follow up with GP
Acute Severe Asthma
Severe asthma defined as:
- PEFR 33-55% predicated or best
- RR >25
- HR >110
- SaO2 90- 95% room air
- Can only speak a few words in one breath
- Mild-moderate use of accessory muscle
- Skin colour: Pallor
- Chest auscultation: Wheeze
Treatment
- Oxygen
- Short-acting Beta2 receptor agonist (ie. Salbutamol with spacer)
- Reassess, Repeat bronchodilator, Reassess, Repeat
- +/- Anticholinergic – Ipratobium bromide (if bronchodilator alone has poor response)
- Reassess, Repeat Ipatropium bromide, Reassess, Repeat
- Oral prednisolone (the earlier given in an attack, the better the outcome) – or IV hydrocortisone if unable to tolerate oral
- Reassess at 1 hour after starting bronchodilator
- Monitor
- Discharge
- +/- IV salbutamol
- +/- IV magnesium sulphate immediately if very severe
- +/- IV aminophylline some patients may respond, give if poor response to initial therapy
- IV fluids – patients are often dehydrated
- Antibiotics – if evidence of infection
Indications for invasive ventilation in asthma
- Coma
- Respiratory arrest
- Exhaustion
- Deteriorating ABG

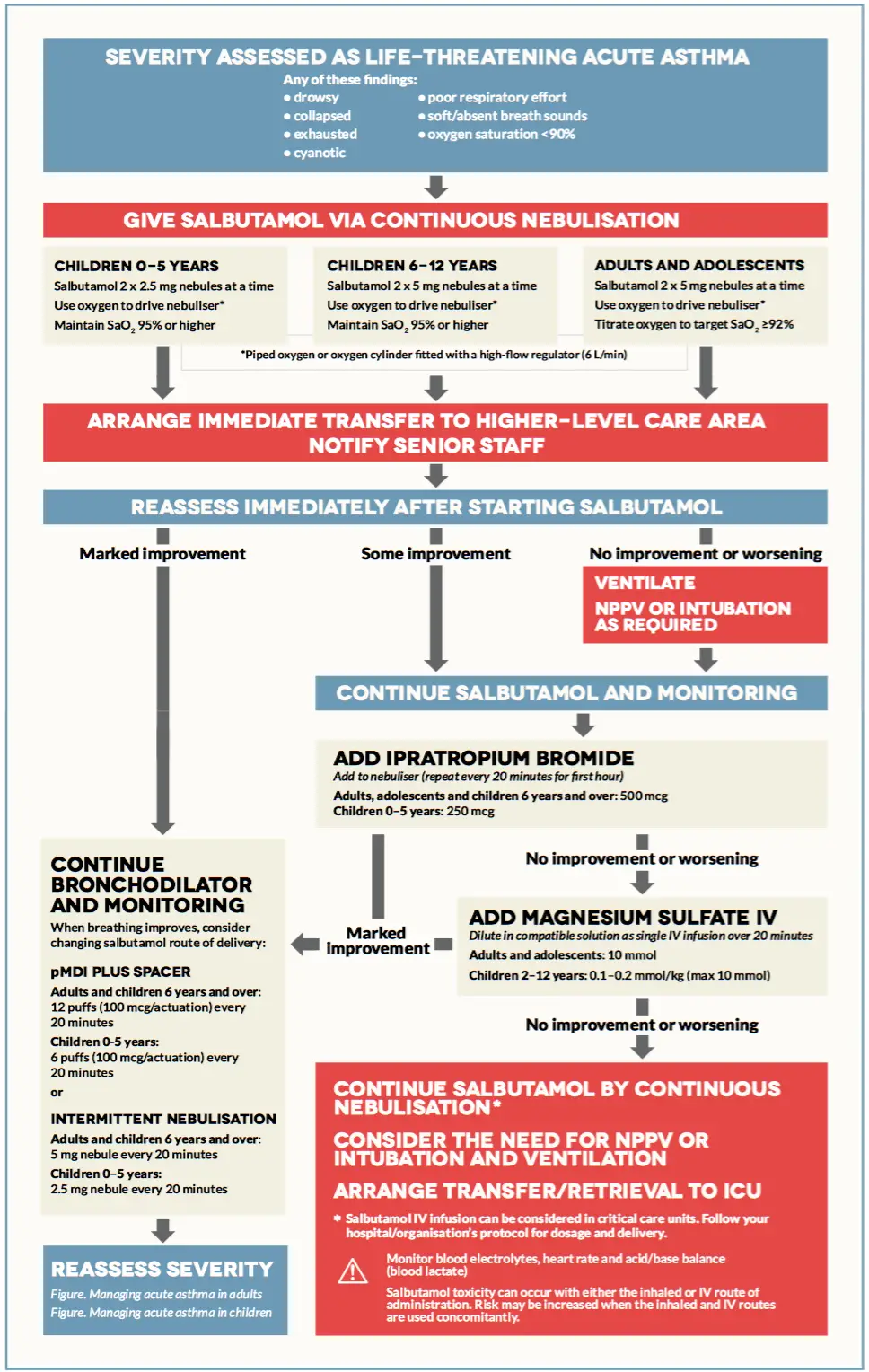
Life-threatening Asthma
Life-threatening asthma any one of:
- PEFR <33%
- SaO2 <90%
- Silent chest (soft/absent breath sounds)
- Cyanosis
- Bradycardia/arrythmia/hypotension
- Exhaustion
- Confusion
- Coma
Mneumonic CHEST for life-threatening asthma: Cynosis, Hypotension and Hypoxia (pO2 <90%), Exhaustion, Silent chest, Tachycardia and Threatening PEF < 33% best or predicted (in those >5yrs old).
Treatment
- β-agonist (Salbutamol via continous nebulisation)
- Anticholinergic – Ippatropium Bromide
- Steroids (the earlier given in an attack, the better the outcome)
- IV salbutamol
- IV magnesium sulphate immediated if very severe
- IV aminophylline some patients may respons, give if poor response to intitial therapy
- +/- Intubation and ventilation
- IV fluids patients are often dehydrated
- Antibiotics only if an infection caused exacerbation
| Indications for assisted ventilation in asthma |
| Coma |
| Respiratory arrest |
| Exhaustion |
| Deteriorating ABG |
Mneumonic O-SHIT-MI for the management of Severe/Life-threatening asthma: Oxygen, Salbutamol, Hydrocortisone (Prednisolone), Ippatropium bromide, Theophylline, Magnesium sulphate, Intubation and ventilation.
Pathogenesis Asthma Exacerbations
Airway obstruction occurs due to a combination of:
- Inflammatory cell infiltration
- Mucus hypersecretion with mucus plug formation
- Smooth muscle contraction
Long-term uncontrolled asthma can lead to air trapping and asthma exacerbations through what is called dynamic hyperinflation.
- Airflow obstruction → Slow expiratory airflow and incomplete gas exhalation dynamic hyperinflation → Patient takes next breath → Gas becomes trapped in alveoli
- Gas becomes trapped in alveoli until the alveoli can not hold any more gas and exhaled volume = inhaled volume → Equilibrium

Mild asthma
- Only most severely obstructed airways collapse
- Collapsed airways with air trapping results in:
- Decreased expiratory reserve volume
- Increased residual volume
As asthma gets more severe
- Expiratory reserve diminishes and this results in profound dyspnoea
Complications of Asthma exacerbations
- Cardiac arrest
- Respiratory failure/arrest
- Hypoxaemia with CNS injury
- Pneumothorax
- Toxicity with medications
- Aspiration/pneumonia
- Nosocomial infection