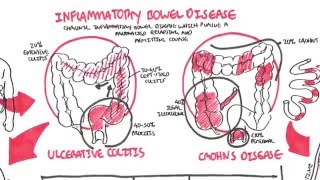
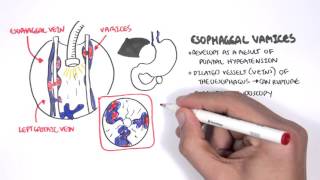
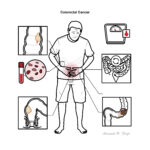
Colorectal Cancer


Colon cancer is the second most commonly diagnosed cancer. 1/12 people will develop bowel cancer before the age of 85. However, there are Survival rates are increasing. Early bowel cancer is cured by surgery alone (screening is important!!). If untreated, or diagnosed when distance metastases are present, >98% pf patients die in <5 years.
Polyps: protuberance into the lumen of normally flat colonic mucosa
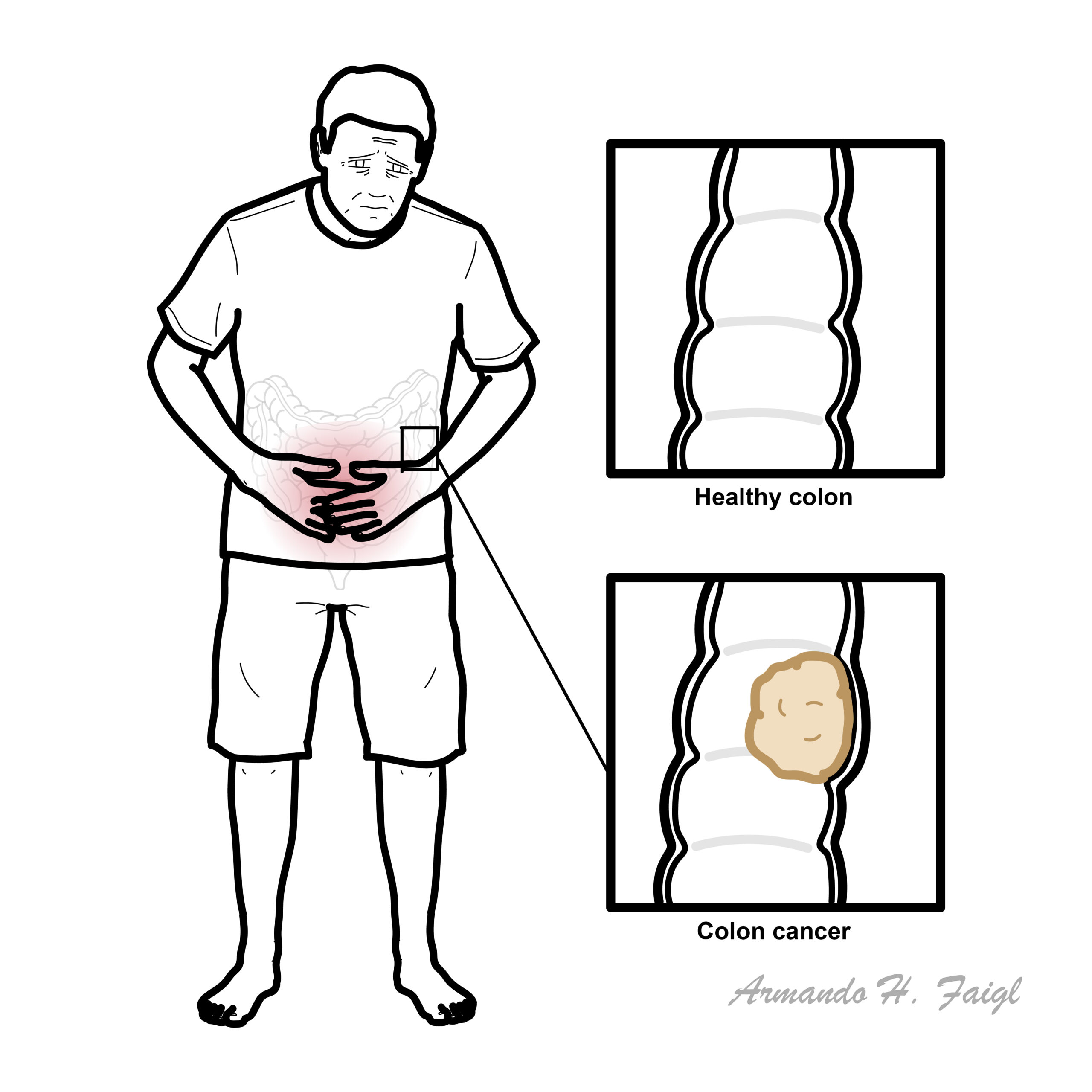
Colorectal Cancer: Cancer of the colon and/or rectum usually at an advanced age. It is an adenoma and the primary site of metastasis is the liver.
Familial Adenomatous Polyposis: autosomal dominant inheritance (mutation of the adenomatous polyposis coli gene), characterised by hundred to thousands of colorectal adenomas usually by age 20.
Lynch Syndrome: autosomal dominant inheritance (mutation of the mismatch repair gene) predisposing one to develop cancer at a younger age.
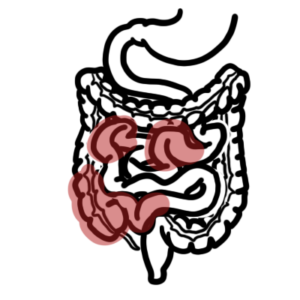
The colon is divided into:
The ascending and descending colon are retroperitoneal, these are immobile. The transverse is mobile and lies within the peritoneal cavity. The transverse colon is supported by the greater omentum superiorly and attaches to the posterior abdominal wall (in front of the retroperitoneal cavity) by the transverse mesocolon.
The transverse colon is attached to the greater curvature of the stomach and first part of the duodenum via the greater omentum. The sigmoid colon is also attached
Main features of large intestine structure:
Blood supply – from superior and inferior mesenteric artery
Autonomic nerve supply
Family and personal history are strong risk factors. Polyposis syndrome including FAP has a 100% chance of developing colon cancer.
Signs and symptoms vary depending on the location of the tumour. 20% of people present at emergency with obstruction of large bowel or perforation.
| CLINICAL PRESENTATION | |||
| Right Colon | Left and Sigmoid Colon | Rectum | |
| Frequency | 20% | 75% | 5% |
| Pathology | Exophytic lesions wit occult bleeding | Annular, invasive lesions | Ulcerating |
| Symptoms | Weight los, weaknes, rarely obstruction | Constipation, change in bowel habits, abdominal pain, rectal bleeding | Obstruction, tenesumus, rectal bleeding |
| Signs | Fe+ deficiency anaemia, QLR mass (10%) | Palpable mass on Digital Rectal Examination | |
Elderly persons who present with iron-deficiency anemia should be investigated for colon cancer.
Occult blood in the stool of a person older than 40 years should be considered colon cancer until proven otherwise. To rule out colon cancer, perform a colonoscopy.
Clinical Examination
For more information: Clinical Presentation of Per-rectal bleeding
Screening for colon cancer is available: FOBT. Done yearly after 50yo (Australia).
Diagnosis Colon cancer is usually diagnosed with colonoscopy and biopsy (takes 1-2 days for pathology results).
Colorectal cancer are primarily adenocarcinoma. Colon cancer can be polyploid, ulcerative, stenosing or infiltrative.
Blumer’s shelf: A firm lump felt in the perirectal pouch on rectal examination. It is a rare physical finding in patients with metastatic adenocarcinoma from the GIT usually the stomach.
Staging CT and PET scan are used for staging colon cancer. The staging system used is TNM which look at the primary tumour, regional lymph node involvement and metastasis. Duke’s staging looks at the 5 year survival rate and this is based on the layers/sites the tumours have invaded.
Duke’s staging (5 year survival rate)
Surgery can be curative if done early with lymphadenectomy. Surgical removal of parts of the colon will depend on site of primary tumour(s). Chemoradiotherapy is also used, chemo agent primarily 5-flurouracil. Finally palliative care if surgery is not an option.
Hand-Foot Syndrome is a side effect for 5-fluorouracil chemotherapy characterised by a tender, symmetrical erythema of the palms and sole of foot.
Prognosis (Based on Dukes) Criteria 5-year survival rates for colorectal cancer are:
Screening
Overview
Other manifestations
Overview
Overview
UpToDate
BestPractice
Oxford Handbook of Clinical Surgery
Toronto Notes 2016












Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.


Discussion