

Chronic Pancreatitis

Overview
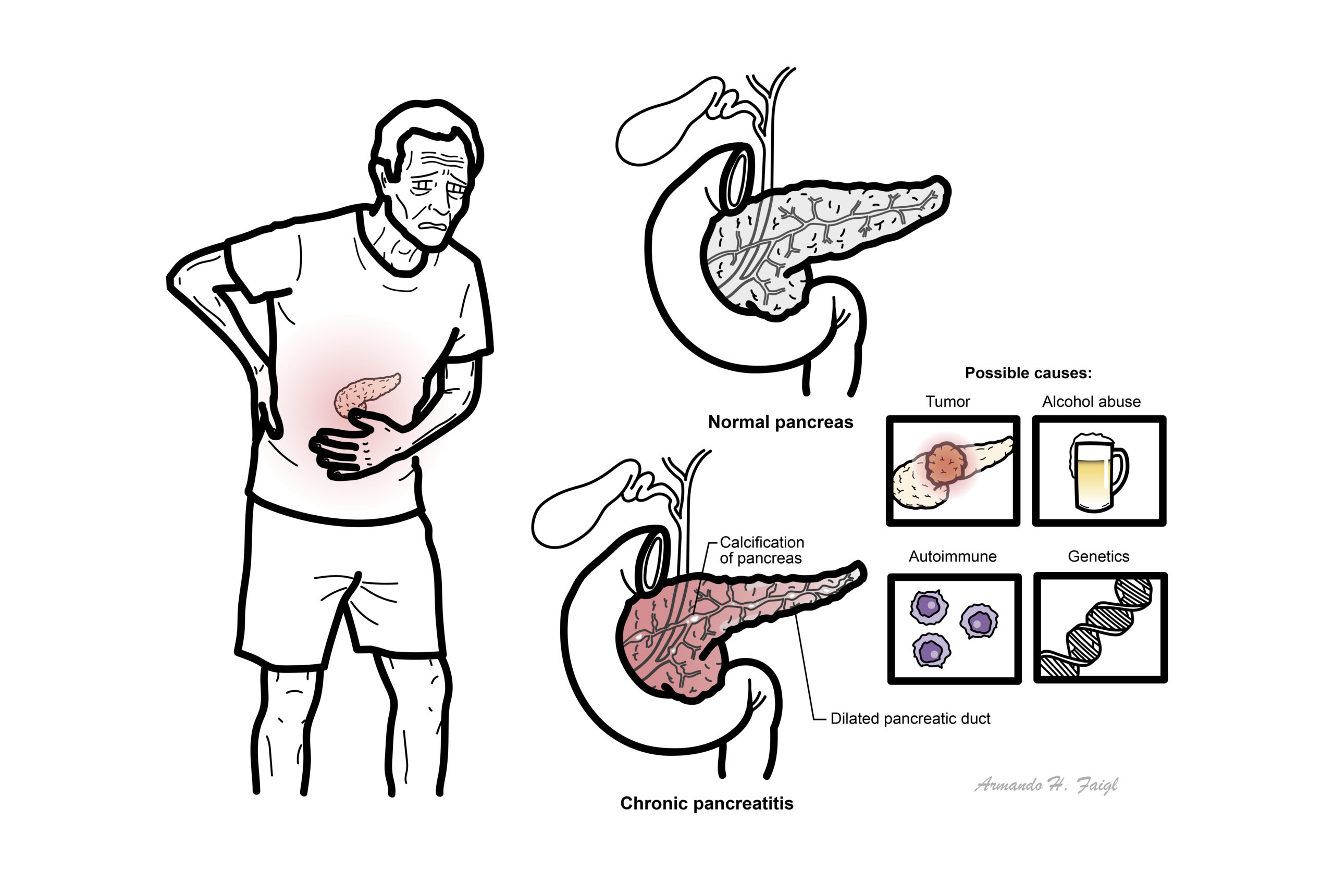
Chronic pancreatitis is a progressive fibro-inflammatory disease of the pancreas that causes irreversible structural damage and eventual loss of exocrine and endocrine pancreatic function. It commonly presents with recurrent or persistent upper abdominal pain and may later cause malabsorption, weight loss and pancreatogenic diabetes. Alcohol exposure and smoking are important causes and accelerators, but genetic, autoimmune, metabolic, anatomical and obstructive disorders must also be considered.
Definition
Pancreatic exocrine insufficiency: inadequate secretion of digestive enzymes and bicarbonate, causing maldigestion, steatorrhoea and nutrient deficiencies.
Type 3c diabetes mellitus: diabetes secondary to pancreatic disease, characterised mainly by reduced insulin secretion.
Pancreatic calcification: calcium deposits within the pancreatic parenchyma or ducts, strongly supporting advanced chronic pancreatitis.
Pancreatic duct stricture: narrowing of the main pancreatic duct that may cause upstream obstruction, duct dilatation and pain.
Pancreatic pseudocyst: encapsulated pancreatic-fluid collection without an epithelial lining, usually developing after pancreatitis.
Pancreatic enzyme replacement therapy—PERT: oral pancreatic enzymes used to treat maldigestion caused by exocrine insufficiency.
Pancreas anatomy and physiology
Pancreatic anatomy
Pancreas extends retroperitoneally across posterior abdominal wall. It means “All (pan) Flesh (Kreas)”. The pancreas consists of the following parts:
- Head
- Neck
- Body
- Tail
The head is encircled by duodenum and tail in contact with spleen. Pancreas has a poorly developed capsule & therefore adjacent structures (common bile duct, duodenum, splenic vein, transverse colon) are commonly involved in inflammatory process.
Blood Supply
- Pancreatic branches of the splenic artery
- Superior pancreaticoduodenal artery
- Inferior pancreaticoduodenal artery
Venous drainage
- Drains with the splenic vein → Superior Mesenteric → Portal vein
Nerve invervation
- Parasympathetic → Vagus nerve → Stimulates pancreatic juice secretion
- Sympathetic
- Head and Neck → Pancreticoduodenal nodes →
- Body and Tail → Pancreaticosplenic nodes →
Embryology
- Fusion of the ventral and doral outpounchings of forgut
Pancreatic physiology exocrine (98%) & endocrine (2%) functions
Exocrine: Pancreatic acinar cells produce digestive enzymes, which are stored in secretory granules. The Pancreatic exocrine secretion is regulated by cephalic, gastric & intestinal stimuli. Acinar cells secrete pancreatic juice made up the enzymes:
- Amylase → Carbohydrate digestion
- Lipase → Lipid digestion after bile has emulsified the fat
- Proteases (MANY!) → Protein digestion
Exocrine section is stimulated by:
- Vagus nerve
- Secretin (hormone)
- Cholecystokinin
Endocrine: Islets of Langerhans – clusters of hormone-producing cells secreted directly into circulation. Endocrine cells of the pancreas:
- Beta cells → Insulin
- Alpha cells → Glucagon
- D cells → Somatostatin.
| Cells of the Pancreas | Secretion | Function |
| Acinar cells secrete enzymes into the duodenum | Nucleases | Breaksdown nucleotides |
| Proteases | Digests Proteins | |
| Lipases | Digests lipids | |
| B-amylase | Digests carbohydrates | |
| Islets of Lagerhan secrete hormones into the bloodstream | Glucagon | Stimulates glucose release into the bloodstream from glucose stores |
| Insulin | Increases cell uptake and storage of glucose |
Aetiology and Risk Factors
A useful classification is TIGAR-O:
Toxic–metabolic
- Chronic heavy alcohol exposure
- Cigarette smoking
- Hypercalcaemia, including hyperparathyroidism
- Hypertriglyceridaemia
- Chronic kidney disease
- Selected medicines or toxins
Smoking independently increases the risk of chronic pancreatitis and accelerates progression.
Idiopathic
- Early-onset idiopathic chronic pancreatitis
- Late-onset idiopathic chronic pancreatitis
- No cause identified after appropriate investigation
Genetic
- PRSS1: hereditary pancreatitis
- CFTR: Cystic firbrosis
Genetic testing should be considered in young patients, those with a family history or unexplained recurrent pancreatitis.
Autoimmune
- Type 1 autoimmune pancreatitis associated with IgG4-related disease
- Type 2 autoimmune pancreatitis, sometimes associated with inflammatory bowel disease
Recurrent or severe acute pancreatitis
- Recurrent gallstone pancreatitis
- Recurrent alcohol-related pancreatitis
- Post-necrotising pancreatitis
- Recurrent acute pancreatitis from another cause
Obstructive
- Pancreas divisum
- Main pancreatic-duct stricture
- Pancreatic or periampullary tumour
- Intraductal papillary mucinous neoplasm
- Post-traumatic or postoperative duct obstruction
Pathophysiology
Pathological features
- The process may affect the whole or part of the gland
- The head tends to be the most severely involved part in chronic alcoholic pancreatitis
- Features of acute pancreatitis may be present (fat necrosis, haemorrhage and/or oedema)
- Chronic inflammatory changes include atropy, duct dilation, microcalcification and intraductal stone formation with cystic changes secondary to ductal occlusion.
Clinical Manifestation
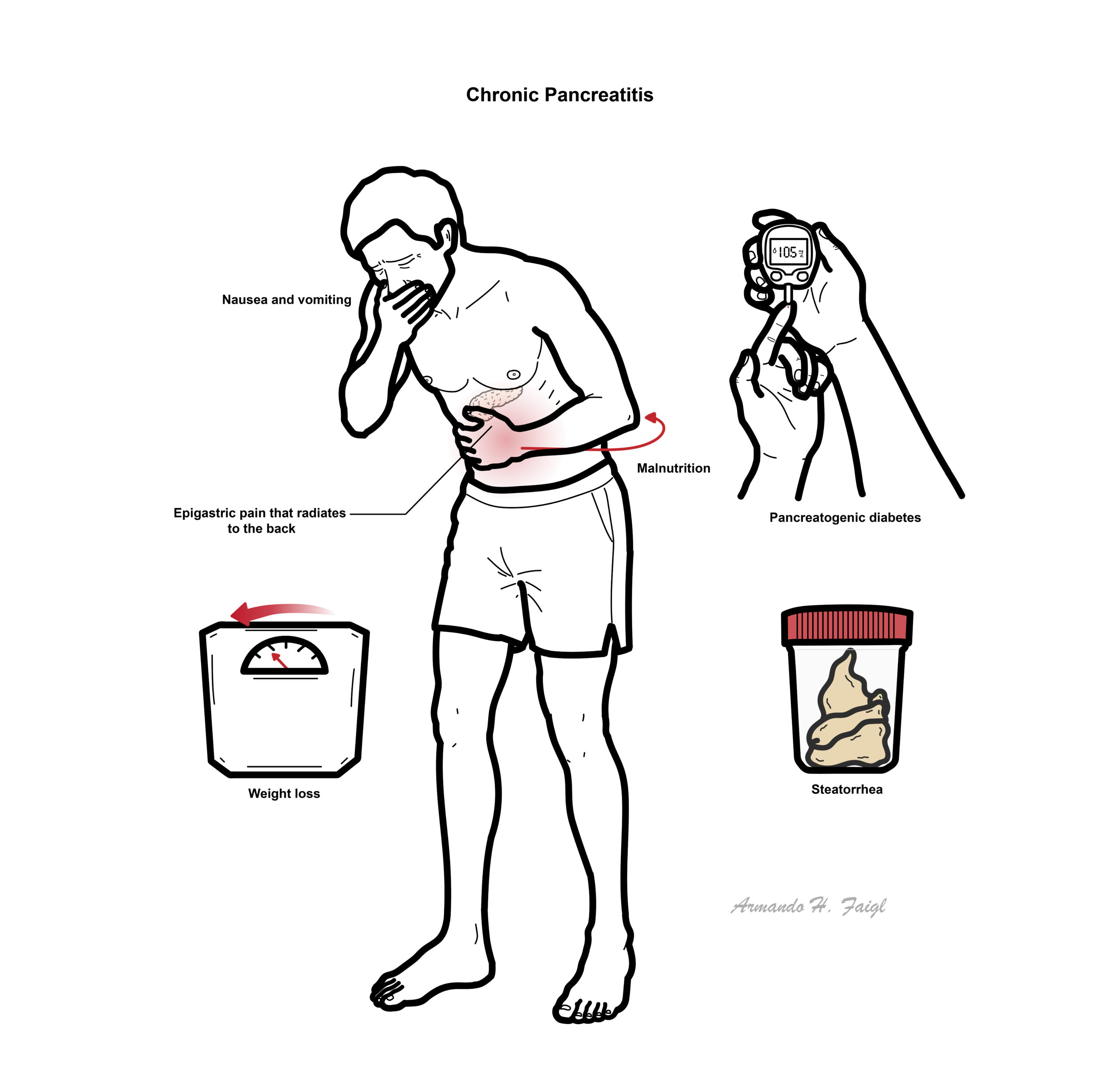
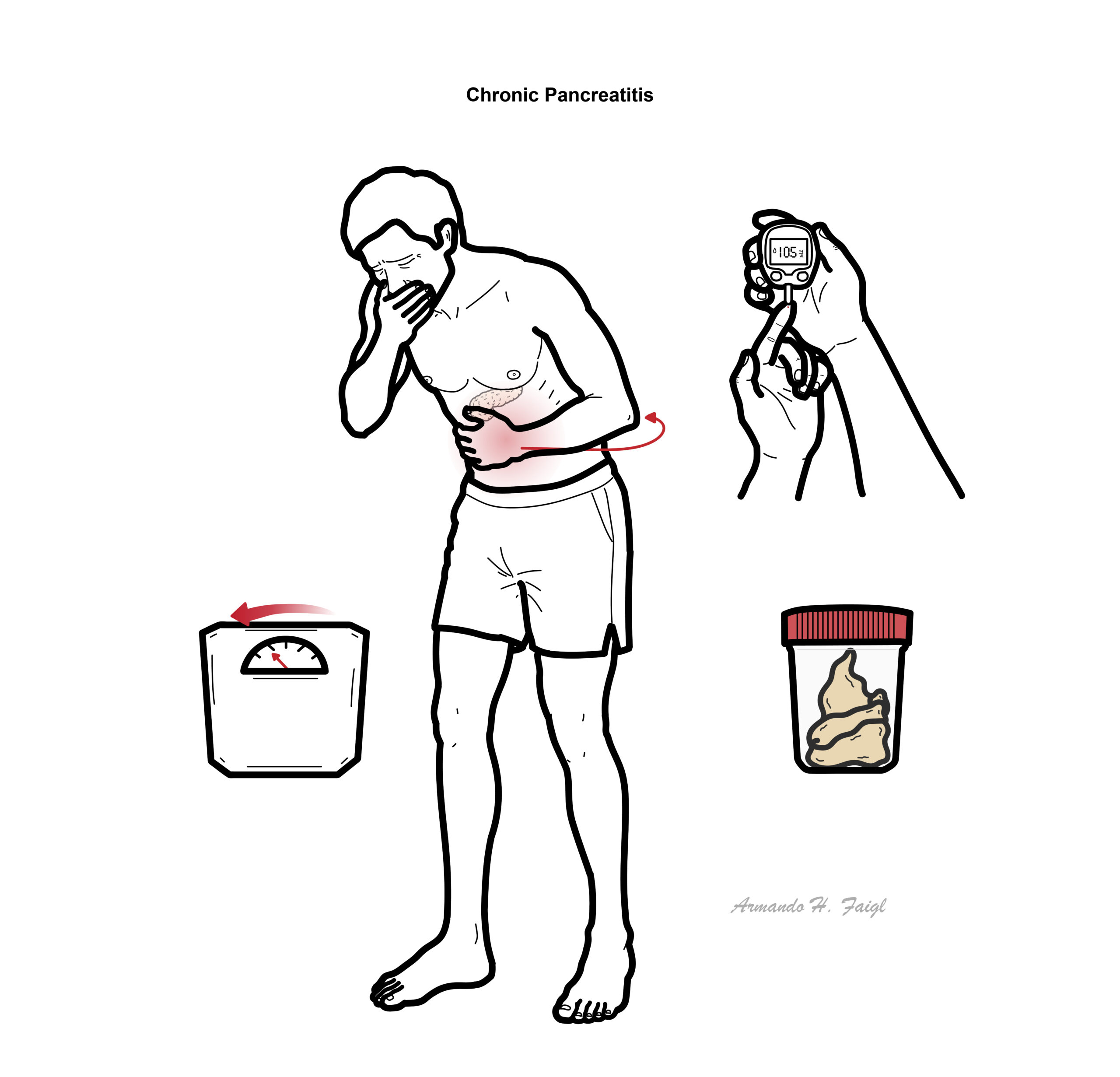
Clinical Presentation of chronic pancreatitis is similar to acute pancreatitis but less severe. This include epigastric pain that may radiate to the back, nausea and vomiting. Patients may present to ED and require opiates. Pain is worse with food and alcohol. Exocrine features of chronic pancreatitis include weight loss and malnutrition (due to malabsorption of macromolecules) and also steatorrhea (due to fat malabsorption).
Pancreatic exocrine insufficiency
Usually develops after substantial loss of exocrine function:
- Steatorrhoea:
- Pale, oily, bulky or difficult-to-flush stools
- Diarrhoea and abdominal bloating
- Excessive flatulence
- Weight loss
- Sarcopenia and malnutrition
- Fat-soluble vitamin deficiencies:
- Vitamins A, D, E and K
- Osteopenia or osteoporosis
Endocrine insufficiency
- Hyperglycaemia
- Type 3c diabetes mellitus
- Polyuria, polydipsia and weight loss
- Unpredictable hypoglycaemia due to reduced glucagon reserve
- Pancreatic cancer
- Acute pancreatitis
- Gallstone disease
- Peptic ulcer disease
- Mesenteric Ischemia
- Triple A (AAA)
- Myocardial infarction
- Irritable bowel syndrome
- Nephrolithiasis (kidney stones)
Diagnosis
Chronic pancreatitis is diagnosed using the clinical presentation together with imaging and pancreatic-function assessment. Serum amylase and lipase may be normal and cannot exclude chronic pancreatitis.
Investigation for underlying cause
- Calcium and triglycerides
- Serum IgG4
Pancreatic-function testing
- Faecal elastase-1: commonly used non-invasive test for exocrine insufficiency.
- <100 micrograms/g strongly supports exocrine insufficiency.
- 100–200 micrograms/g is indeterminate.
- A watery stool sample may give a falsely low result.
- Faecal fat testing is rarely required but can quantify fat malabsorption.
- Direct secretin-stimulation tests are more sensitive but have limited availability.
Clinical response to pancreatic enzymes should not be used alone to establish the diagnosis of exocrine insufficiency.
Imaging
Contrast-enhanced CT pancreas
Common first-line structural investigation. Findings may include:
- Pancreatic calcifications
- Glandular atrophy
- Main pancreatic-duct dilatation
- Ductal stones or strictures
- Pseudocyst
- Inflammatory mass
- Biliary or duodenal obstruction
MRI and MRCP
- Assesses the pancreatic parenchyma and ductal anatomy.
- May identify duct strictures, side-branch abnormalities and fluid collections.
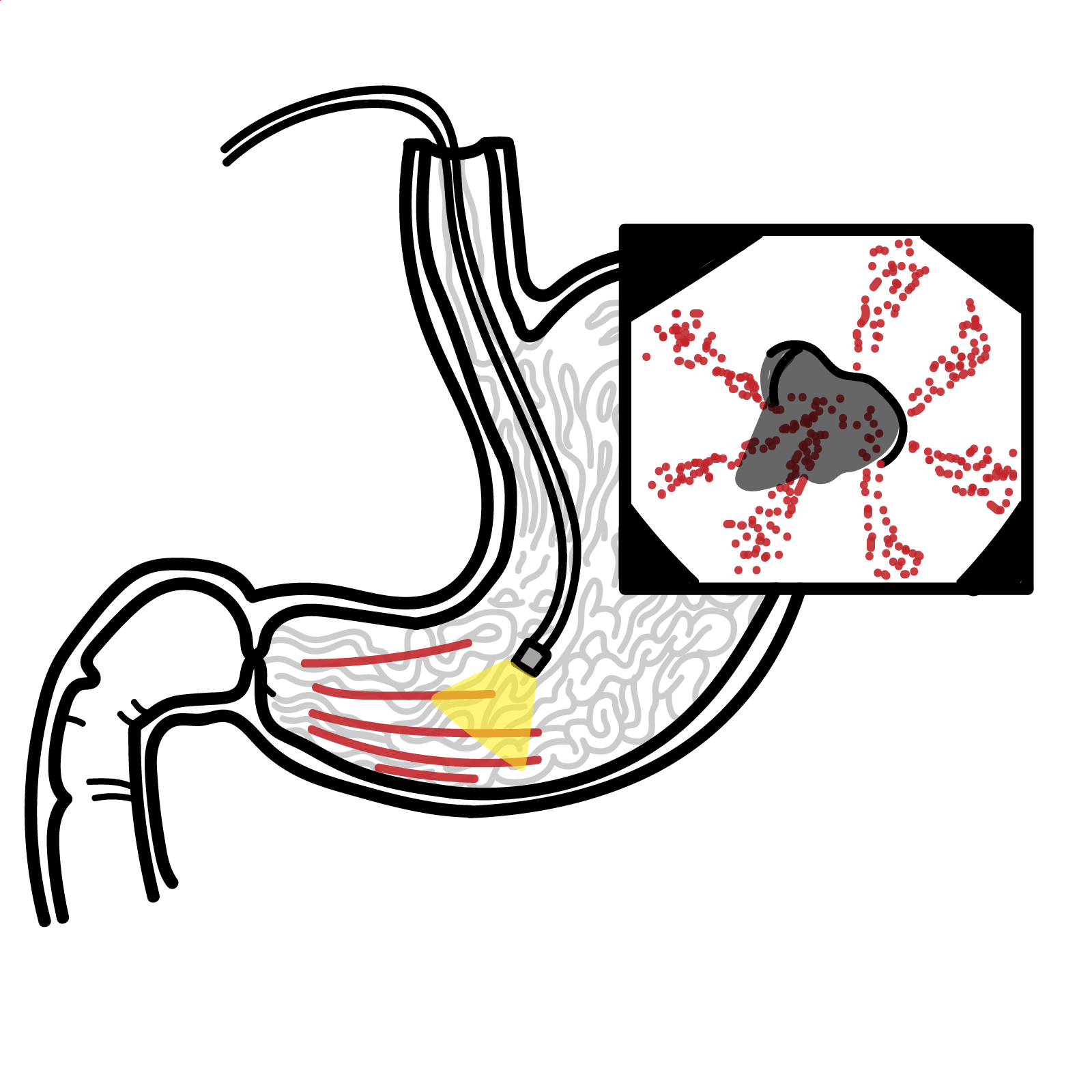
Endoscopic ultrasound
- Useful when CT or MRI is non-diagnostic but clinical suspicion remains high.
- Detects subtle parenchymal and ductal abnormalities.
- Allows tissue sampling when pancreatic malignancy or autoimmune pancreatitis is suspected.
Assessment for complications
- CT, MRI or EUS for a pancreatic mass or pseudocyst.
- MRCP or ERCP for biliary or pancreatic-duct obstruction.
- CT angiography for suspected pseudoaneurysm or haemorrhage.
- Bone mineral-density testing every 2 years in adults.
- HbA1c at least every 6 months.
- Assess exocrine function and nutritional status at least annually.
Treatment
Management involve prevention of cause/progressive damage by stoping alcohol and smoking. Encourage diet rich in antioxidant. Controlling symptoms and complication involve dietary modification (low fat), pancreatic enzyme supplements, analgesia (may require opiates), insulin (for diabetes if develops). Surgical management includes percutaneous or endoscopic drainage to drain excess fluid in the pancreas that is causing obstruction. Pancreaticduodenectomy is performed to remove possible causes and complications.
Complications and Prognosis
Resectional surgery is associated with increasing risk of exocrine and endocrine pancreatic failure and high risk of complications
Complications
- Pseuodocyst
- Obstruction
- Fistula
- Infections
- Portal hypertension
- Diabetes Mellitus
- Pancreatic calcification
- Opiod addiction
- Generally, pain decreases or disappears over time, regardless of aetiology
- Ten-year survival after diagnosis is 20% to 30% lower than the general population.
References
- Gardner TB, Adler DG, Forsmark CE, Sauer BG, Taylor JR, Whitcomb DC. ACG clinical guideline: chronic pancreatitis. Am J Gastroenterol. 2020;115(3):322–339. doi:10.14309/ajg.0000000000000535.
- National Institute for Health and Care Excellence. Pancreatitis. NICE guideline NG104. London: NICE; 2018. Updated 2020.
- Löhr JM, Dominguez-Munoz E, Rosendahl J, Besselink M, Mayerle J, Lerch MM, et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis—HaPanEU. United European Gastroenterol J. 2017;5(2):153–199. doi:10.1177/2050640616684695.
- Whitcomb DC, Buchner AM, Forsmark CE. AGA clinical practice update on the epidemiology, evaluation and management of exocrine pancreatic insufficiency: expert review. Gastroenterology. 2023;165(5):1292–1301. doi:10.1053/j.gastro.2023.07.007.
- Shimizu K, Ito T, Irisawa A, Ohtsuka T, Ohara H, Kanno A, et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2021. J Gastroenterol. 2022;57(10):709–724. doi:10.1007/s00535-022-01911-6.






Members only discussions coming soon…