

Acute Pancreatitis
Overview
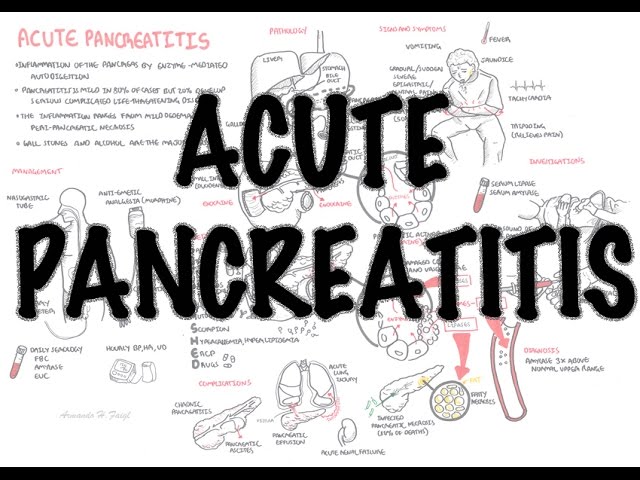
Acute pancreatitis is sudden inflammation of the pancreas caused by premature activation of pancreatic digestive enzymes within the gland. It ranges from a mild, self-limiting illness to severe necrotising pancreatitis with persistent organ failure. The most common causes are gallstones and alcohol, although hypertriglyceridaemia, medicines, procedures and metabolic disorders are also important.

Definition
Acute Pancreatitis: An inflammatory process in which pancreatic enzymes are activated and cause autodigestion of the gland.
Chronic Pancreatitis: Irreversible damage causing fibrosis and scarring to the pancreas, resulting in exocrine and endocrine dysfunction
Pancreatic pseudocyst: Cystic space within the pancreas not lined by epithelial cells, often associated with chronic pancreatitis.
Interstitial oedematous pancreatitis: pancreatic inflammation and oedema without tissue necrosis.
Necrotising pancreatitis: necrosis involving pancreatic tissue, surrounding tissue or both.
Pancreatic necrosis: non-viable pancreatic or peripancreatic tissue.
Infected necrosis: bacterial or fungal infection within necrotic pancreatic tissue.
Pancreas Anatomy and Physiology
Pancreatic anatomy
Pancreas extends retroperitoneally across posterior abdominal wall. It means “All (pan) Flesh (Kreas)”. The pancreas consists of the following parts:
- Head
- Neck
- Body
- Tail
The head is encircled by duodenum and tail in contact with spleen. Pancreas has a poorly developed capsule & therefore adjacent structures (common bile duct, duodenum, splenic vein, transverse colon) are commonly involved in inflammatory process.
Blood Supply
- Pancreatic branches of the splenic artery
- Superior pancreaticoduodenal artery
- Inferior pancreaticoduodenal artery
Venous drainage
- Drains with the splenic vein → Superior Mesenteric → Portal vein
Nerve invervation
- Parasympathetic → Vagus nerve → Stimulates pancreatic juice secretion
- Sympathetic
- Head and Neck → Pancreticoduodenal nodes →
- Body and Tail → Pancreaticosplenic nodes →
Embryology
- Fusion of the ventral and doral outpounchings of forgut
Pancreatic physiology exocrine (98%) & endocrine (2%) functions
Exocrine: Pancreatic acinar cells produce digestive enzymes, which are stored in secretory granules. The Pancreatic exocrine secretion is regulated by cephalic, gastric & intestinal stimuli. Acinar cells secrete pancreatic juice made up the enzymes:
- Amylase → Carbohydrate digestion
- Lipase → Lipid digestion after bile has emulsified the fat
- Proteases (MANY!) → Protein digestion
Exocrine section is stimulated by:
- Vagus nerve
- Secretin (hormone)
- Cholecystokinin
Endocrine: Islets of Langerhans – clusters of hormone-producing cells secreted directly into circulation. Endocrine cells of the pancreas:
- Beta cells → Insulin
- Alpha cells → Glucagon
- D cells → Somatostatin.
| Cells of the Pancreas | Secretion | Function |
| Acinar cells secrete enzymes into the duodenum | Nucleases | Breaksdown nucleotides |
| Proteases | Digests Proteins | |
| Lipases | Digests lipids | |
| B-amylase | Digests carbohydrates | |
| Islets of Lagerhan secrete hormones into the bloodstream | Glucagon | Stimulates glucose release into the bloodstream from glucose stores |
| Insulin | Increases cell uptake and storage of glucose |
Aetiology and Risk Factors
Aetiology
The most common cause of acute pancreatitis is gallstones (60%) and alcohol (30%). Many are idopathic. Good acronym to remember is I-GETSMASHED.
I – Idiopathic
G – Gallstones
E – Ethanol (alcohol)
T – Trauma
S – Steroids
M – Mumps
A – Autoimmune pancreatitis
S – Scorpion sting
H – Hypertriglyceridaemia and hypercalcaemia
E – ERCP
D – Drugs
Important drug causes include azathioprine, 6-mercaptopurine, valproate, tetracyclines, thiazide diuretics and didanosine.
| Risk Factors |
| Middle aged |
| Gallstones |
| Alcohol |
| Hypertriglyceridaemia |
| MedicationsAzathioprineThiazide diureticsFurosemide |
| HIV/AIDS |
| Endoscopic retrograde cholangiopancreatography |
| Trauma |
| SLE |
| Sjogren’s syndrome |
Pathophysiology
- A pancreatic insult causes premature conversion of trypsinogen to active trypsin within pancreatic acinar cells.
- Activated enzymes begin digesting pancreatic tissue, causing inflammation, oedema and cellular injury.
- Local inflammation may damage pancreatic blood vessels and surrounding tissues, producing haemorrhage or necrosis.
- Inflammatory cytokines can enter the circulation and produce systemic inflammatory response syndrome—SIRS.
- Severe systemic inflammation may cause shock, acute kidney injury, acute respiratory distress syndrome and multiorgan failure.
- Necrotic tissue may initially be sterile but can later become infected by organisms translocating from the gastrointestinal tract.
Clinical Manifestation
Clinical Presentation
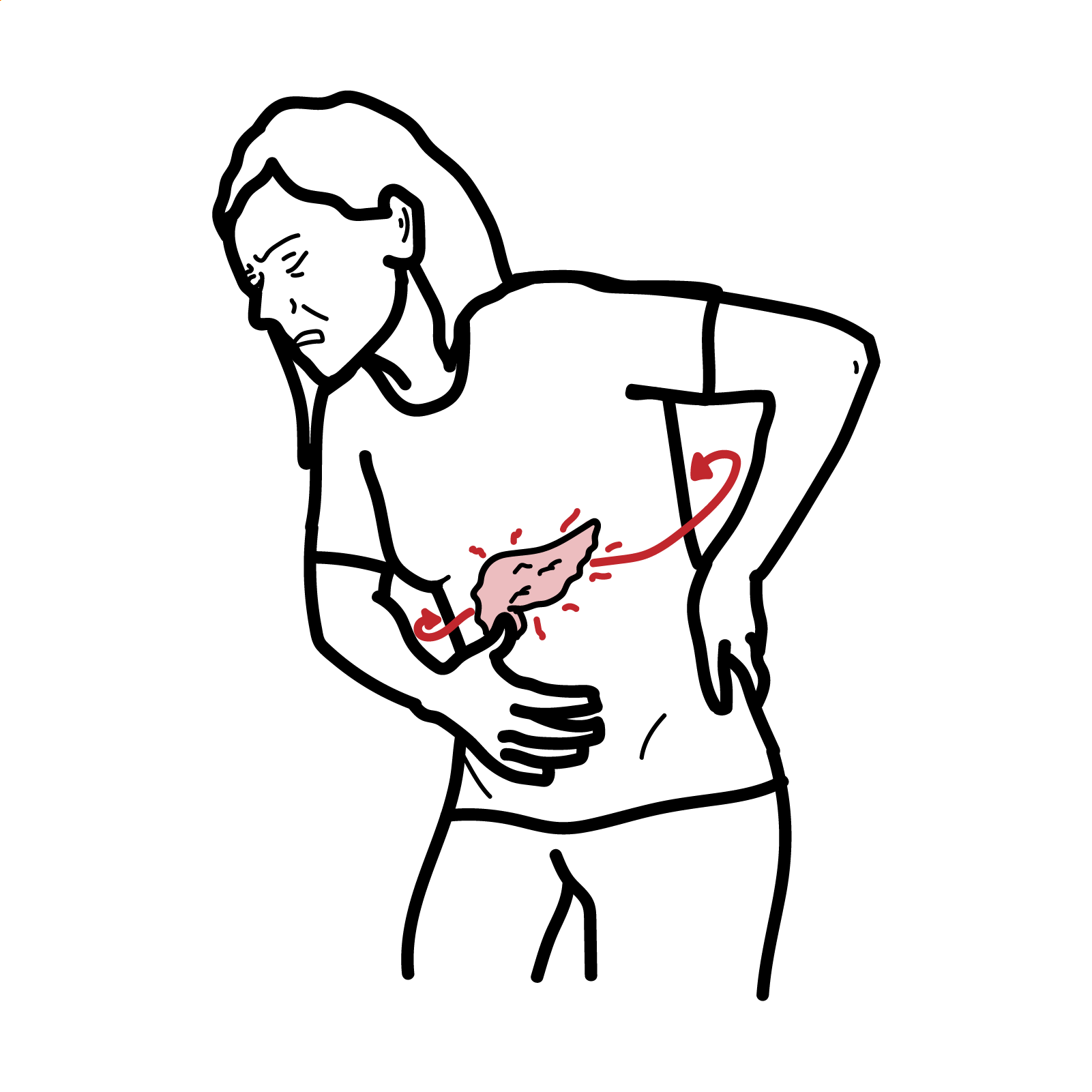
- Sudden, persistent, severe epigastric pain
- Pain commonly radiates through to the back
- Pain may improve when sitting forward
- Nausea and vomiting
- Abdominal distension
- Reduced appetite
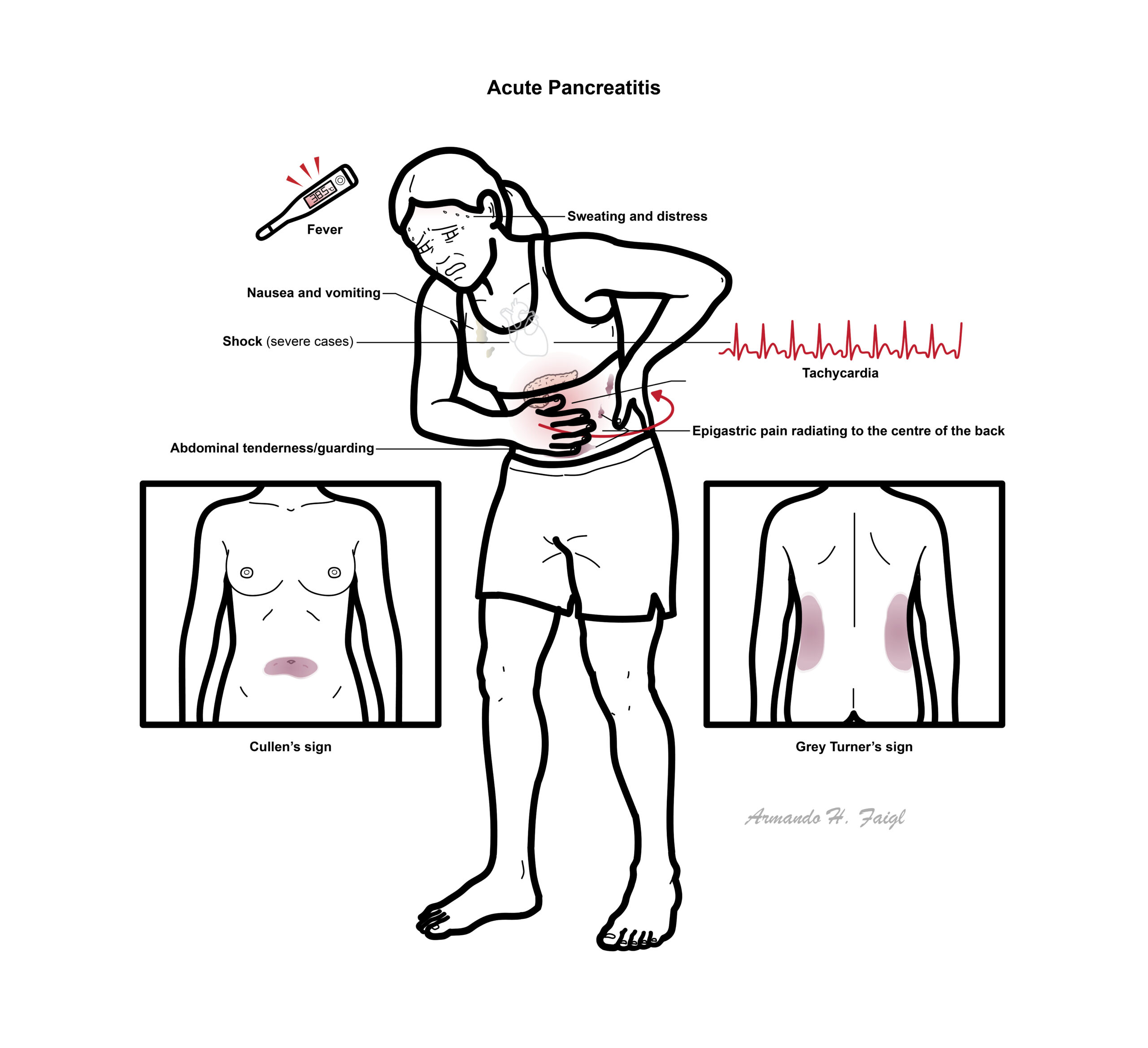
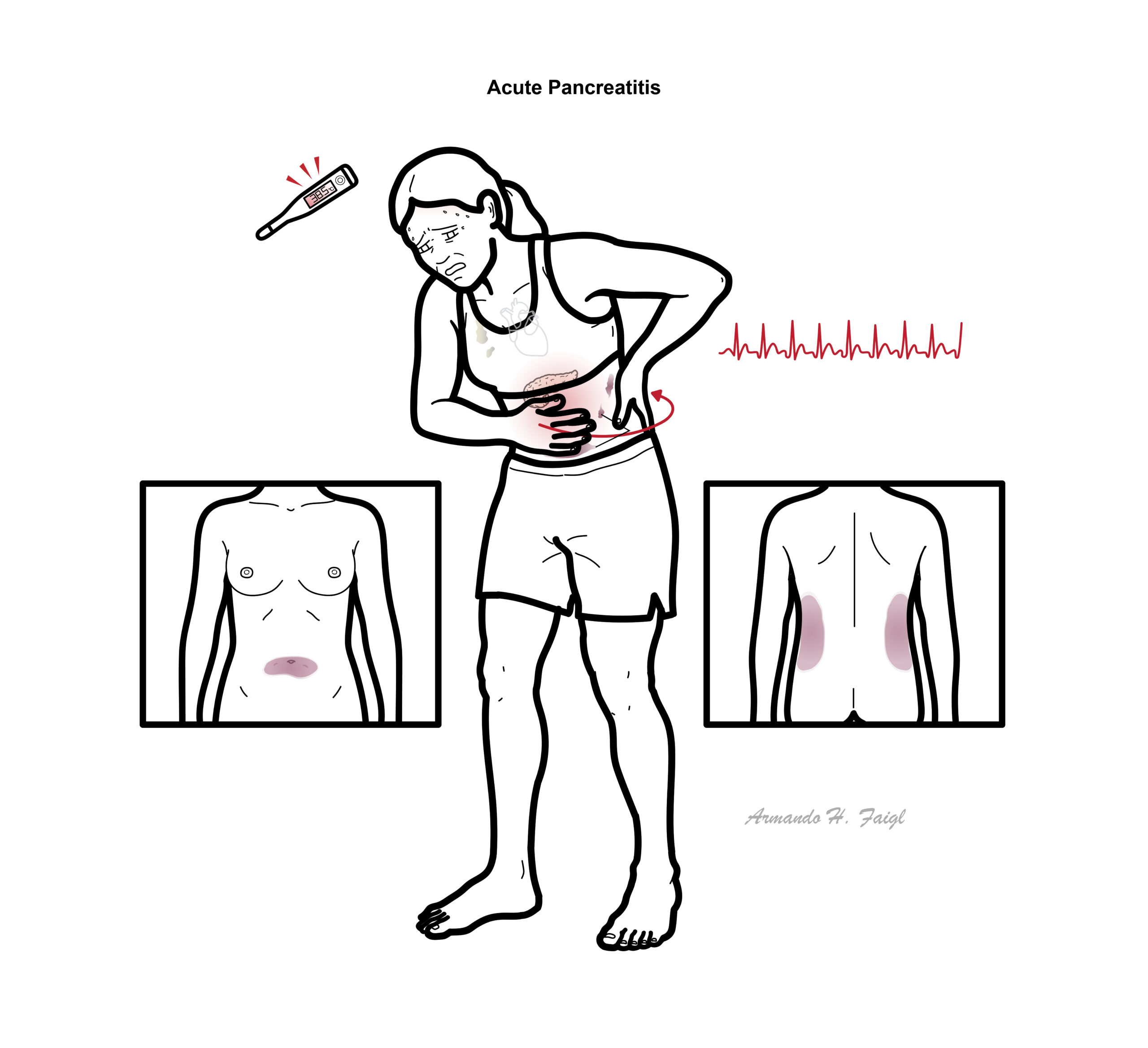
- Fever
- Dyspnoea in severe disease
Clinical Examination
- Epigastric or generalised abdominal tenderness
- Guarding
- Reduced bowel sounds or ileus
- Tachycardia
- Fever
- Dehydration
- Hypotension
- Tachypnoea or hypoxaemia
- Jaundice may suggest gallstone obstruction
- Rare signs of retroperitoneal haemorrhage:
- Cullen sign: periumbilical bruising
- Grey Turner sign: flank bruising
Severe disease may present with shock, confusion, respiratory distress or reduced urine output.
- Peptic Ulcer disease
- Intestinal Obstruction
- Triple A (AAA)
- Gall stone disease
- Viral gastroenteritis
- Myocardial Infarction
Diagnosis
Should be suspected in a patient with acute onset of a persistent, severe, epigastric pain with tenderness on palpation. Requires the presence of 2 of the following 3 criteria:
- Acute onset of persistent, severe, epigastric pain often radiating to the back.
- Elevation in serum lipase or amylase to 3 times or greater than the upper limit of normal.
- Characteristic findings of AP on imaging (CT, MRI, transabdominal ultrasound).
Amylase is not specific to the pancreas. It can be elevated in gastrointestinal ischemia with infarction or perforation, vomiting associated with pancreatitis can cause elevated amylase of salivary origin. Elevated serum lipase level is more specific than is amylase to pancreatic origin and remains elevated longer than does amylase.
Imaging
- Abdominal ultrasound: first-line investigation for gallstones and biliary-duct dilatation.
- Contrast-enhanced CT:
- Diagnosis remains uncertain
- Severe disease or complications are suspected
- The patient fails to improve after approximately 48–72 hours
- Assesses necrosis, collections and alternative diagnoses
- MRI/MRCP: useful for biliary obstruction, small common bile-duct stones or when CT contrast is unsuitable.
- Endoscopic ultrasound: may identify microlithiasis, small bile-duct stones, pancreatic lesions or causes of recurrent unexplained pancreatitis.
Classification: severity
Glasgow Imrie criteria (PANCREAS)
- PaO2 <8kPa
- Age >55y – Poorer Prognosis
- Neutrophils/WCC >15000
- Corrected Calcium – Increased protease in serum chelates serum calcium
- Raised blood urea – Increased protease in serum leads to increase in protein breakdown leading to ureamia
- Elevated Enzymes – LFT dysfunction (specifically in gall stone causes)
- Albumin – Increased protease leads to albumin breakdown and shift of albumin to interstitium cause of increased in permeabiliy.
- Sugar, blood glucose >10mmol/L – beta cell damage
Grades of severity
- Mild acute pancreatitis
- No organ failure
- No local or systemic complications
- Moderately severe acute pancreatitis
- Organ failure that resolves within 48 h (transient organ failure) and/or
- Local or systemic complications without persistent organ failure
- Severe acute pancreatitis
- Persistent organ failure (>48 h)
- Single organ failure
- Multiple organ failure
- Persistent organ failure (>48 h)
Treatment
Initial management
- Admit for observation and supportive management.
- ABC assessment and regular monitoring.
- Supplemental oxygen if hypoxaemic.
- Adequate analgesia, including opioid analgesia when required.
- Antiemetics.
- Correct electrolyte and glucose abnormalities.
- Monitor:
- Heart rate and blood pressure
- Oxygen saturation
- Mental state
- Urine output
- Urea, creatinine and haematocrit
- Evidence of organ failure.
Intravenous fluids
- Use goal-directed crystalloid resuscitation, particularly during the first 24 hours.
- Lactated Ringer solution is generally preferred by contemporary ACG guidance.
- Reassess frequently to avoid both inadequate resuscitation and fluid overload.
- Use additional caution in older patients and those with cardiac or renal disease.
- Excessively aggressive fluid administration can cause pulmonary oedema, abdominal compartment syndrome and other complications.
Nutrition
- Start oral feeding within 24–48 hours as tolerated rather than routinely keeping the patient nil by mouth.
- A low-fat solid or soft diet may be commenced without first progressing through clear fluids.
- If oral feeding is not possible, use enteral tube feeding.
- Nasogastric and nasojejunal feeding are both acceptable.
Antibiotics
- Do not give prophylactic antibiotics for sterile necrosis or predicted severe pancreatitis.
- Antibiotics are indicated for:
- Infected pancreatic necrosis
- Acute cholangitis
- Pneumonia, urinary infection or another confirmed extrapancreatic infection
- Sepsis where bacterial infection is suspected
Specific treatment based on cause
- Biliary pancreatitis/gallstone pancreatitis
- +/- ERCP
- +/- Cholecystectomy
- Mild gallstone pancreatitis: laparoscopic cholecystectomy during the same hospital admission, preferably before discharge.
- Severe or necrotising gallstone pancreatitis: surgery is generally delayed until acute inflammation and significant collections have improved or stabilised.
- Cholecystectomy reduces recurrent pancreatitis and other gallstone-related complications.
- Alcohol-related pancreatitis
- Alcohol cessation.
- Thiamine replacement where indicated.
- Hypertriglyceridaemic pancreatitis
- IV fluids, analgesia and early nutrition as with other causes.
- Control marked hyperglycaemia.
- Insulin infusion may be used in selected patients with severe hypertriglyceridaemia, particularly with diabetes.
- Long-term management includes triglyceride-lowering therapy, diabetes control, dietary intervention and avoidance of alcohol.
- Plasmapheresis is generally reserved for highly selected severe or refractory cases.
- Pancreatic necrosis and collections
- Most sterile necrosis is managed without intervention.
- Infected necrosis or symptomatic collections may require a step-up approach:
- Antibiotics where infection is present
- Endoscopic or percutaneous drainage
- Minimally invasive necrosectomy if drainage is inadequate
- Open surgery only when less invasive treatment fails or is unsuitable
Complications and Prognosis
Local complications
- Acute peripancreatic fluid collection
- Pancreatic pseudocyst
- Walled-off necrosis
- Infected pancreatic necrosis
- Pancreatic duct disruption
- Pleural effusion or pancreaticopleural fistula
- Gastrointestinal or biliary obstruction
- Splenic, portal or mesenteric venous thrombosis
- Pseudoaneurysm and major haemorrhage
- Bowel ischaemia, necrosis or fistula
Systemic complications
- SIRS and sepsis
- Hypovolaemic or distributive shock
- Acute respiratory distress syndrome
- Acute kidney injury
- Disseminated intravascular coagulation
- Venous thromboembolism.
Long-term complications
- Recurrent acute pancreatitis
- Chronic pancreatitis
- Chronic abdominal pain
- Pancreatic exocrine insufficiency
- Diabetes mellitus from endocrine insuffiency
Prognosis
- Most patients have mild interstitial pancreatitis and recover within several days with supportive treatment.
- Prognosis worsens significantly with:
- Persistent organ failure
- Infected pancreatic necrosis
- Older age or frailty
- Obesity
- Renal, respiratory or cardiovascular disease
- Delayed recognition of deterioration
- Mild pancreatitis usually resolves without permanent pancreatic dysfunction.
- Necrotising pancreatitis may require prolonged admission, repeated procedures and rehabilitation.
- Recurrence risk depends on whether the underlying cause is corrected, such as cholecystectomy for gallstones or abstinence from alcohol.
References
- Tenner S, Vege SS, Sheth SG, Sauer B, Yang A, Conwell DL, et al. American College of Gastroenterology Guidelines: management of acute pancreatitis. Am J Gastroenterol. 2024;119(3):419–437. doi:10.14309/ajg.0000000000002645.
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779.
- Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN. American Gastroenterological Association Institute guideline on initial management of acute pancreatitis. Gastroenterology. 2018;154(4):1096–1101. doi:10.1053/j.gastro.2018.01.032.
- Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14:27. doi:10.1186/s13017-019-0247-0.
- National Institute for Health and Care Excellence. Pancreatitis. NICE guideline NG104. London: NICE; 2018. Updated 2020.










Members only discussions coming soon…