

Ruptured Abdominal Aortic Aneurysm
Overview
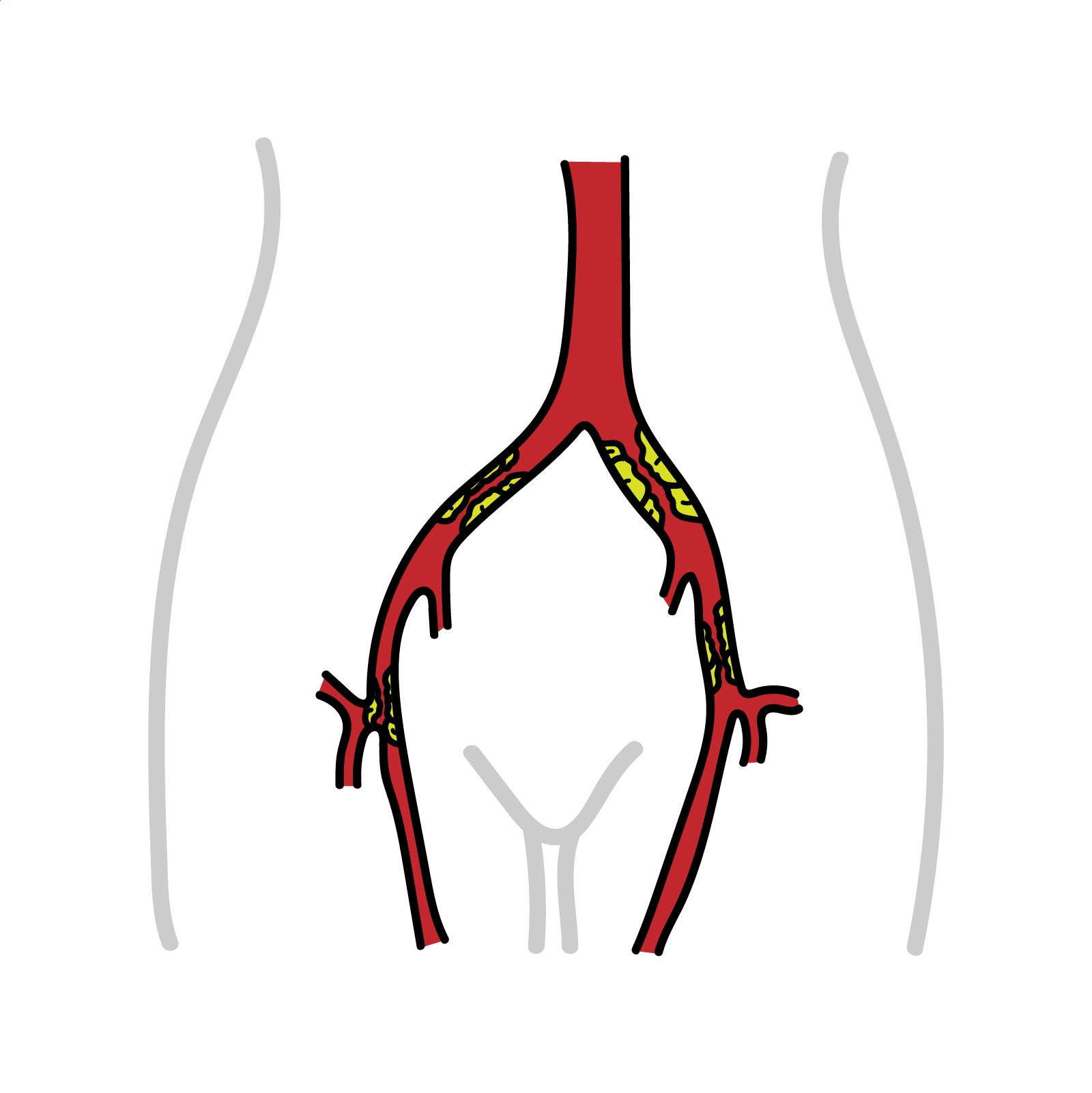
Abdominal Aortic Aneurysm, also known as AAA, is a permanent dilation of the abdominal aorta with a diameter of >1.5 times of the expected diameter. The adopted diameter that indicates AAA is 3cm or more. AAA is strongly associated with smoking and increasing age. Most of these aneurysms are fusiform and originate below the renal arteries. Rupture is associated with an overall mortality rate of 90% and 50% for those reaching hospital. Screening men over 65 reduces AAA-related mortality. Patients diagnosed with small AAA are managed with ultrasound surveillance and cardiovascular risk reduction. Patients with indications for AAA repair should be referred promptly to a vascular surgeon.1 2
Definition
Aneurysm: an artery that has enlarged to greater than 1.5 times the expected diameter.
True Aneurysm: The aneurysm is bound by all three layers of the vessel wall (intima, media and adventitia). The wall may be attenuated.
False Aneurysm: Occurs when a blood vessel wall is injured, and the blood is contained by the surrounding tissues creating an apparent dilatation of vessel.
Aortic dissection: occurs when a tear in the tunica intima of the aorta causes blood to flow between the layers of the wall of the aorta, forcing the layers apart.
Abdominal aorta originates at T12 as it passes through the diaphragm
It bifurcates into the right and left common iliac arteries at L4
Branches of the descending abdominal aorta:
| Branch | Vertebral level of origin | Region of supply |
| Inferior phrenic | T12 | Inferior diaphragm, adrenal glands |
| Coeliac trunk | T12/L1 | Foregut |
| Superior mesenteric | L1 | Midgut |
| Middle suprarenal | L1 | Adrenal glands |
| Renal | L1/L2 | Kidneys, adrenal glands |
| Gonadal | L2 | Gonads (testes/ovaries) |
| Inferior mesenteric | L3 | Hindgut |
| Median sacral | Superior to bifurcation (L4) | Lumbar vertebrae, sacrum |
| Lumbar arteries | L1-L4 | Posterior abdominal wall, spinal cord |
Aetiology & Risk Factors
- Smoking (most significant risk factor)
- Older age
- Male sex (but women rupture at smaller diameters)
- Family history
- Atherosclerosis
- Hypertension
- Hypercholesterolemia
- Other vascular aneurysm 3
Pathophysiology
↓
Chronic aortic wall inflammation
↓
Proteolytic imbalance – Increased Matrix metalloproteinases
↓
Elastin and collagen breakdown + smooth muscle apoptosis
↓
Aortic wall weakening
↓
Progressive dilation
↓
Eventually wall stress exceeds vessel strength and causes rupture
Classification
Anatomical:
- Suprarenal: involves origins of one or more visceral arteries but does not extend into the chest
- Pararenal: at the origin of the renal artery; the aorta at the level of superior mesenteric artery is not aneurysmal
- Juxtarenal: originates just beyond the renal arteries (<10mm)
- Infrarenal: originates distal to the renal arteries
Most AAA are located infrarenally due to less elastin in the aortic wall and lack of vasa vasorum, which makes tunica media more susceptible to ischaemia.
Diameter:
- Small: <4 cm
- Medium: between 4.0 and 5.5 cm
- Large: >5.5 cm
- Very large: 6 cm or more 3
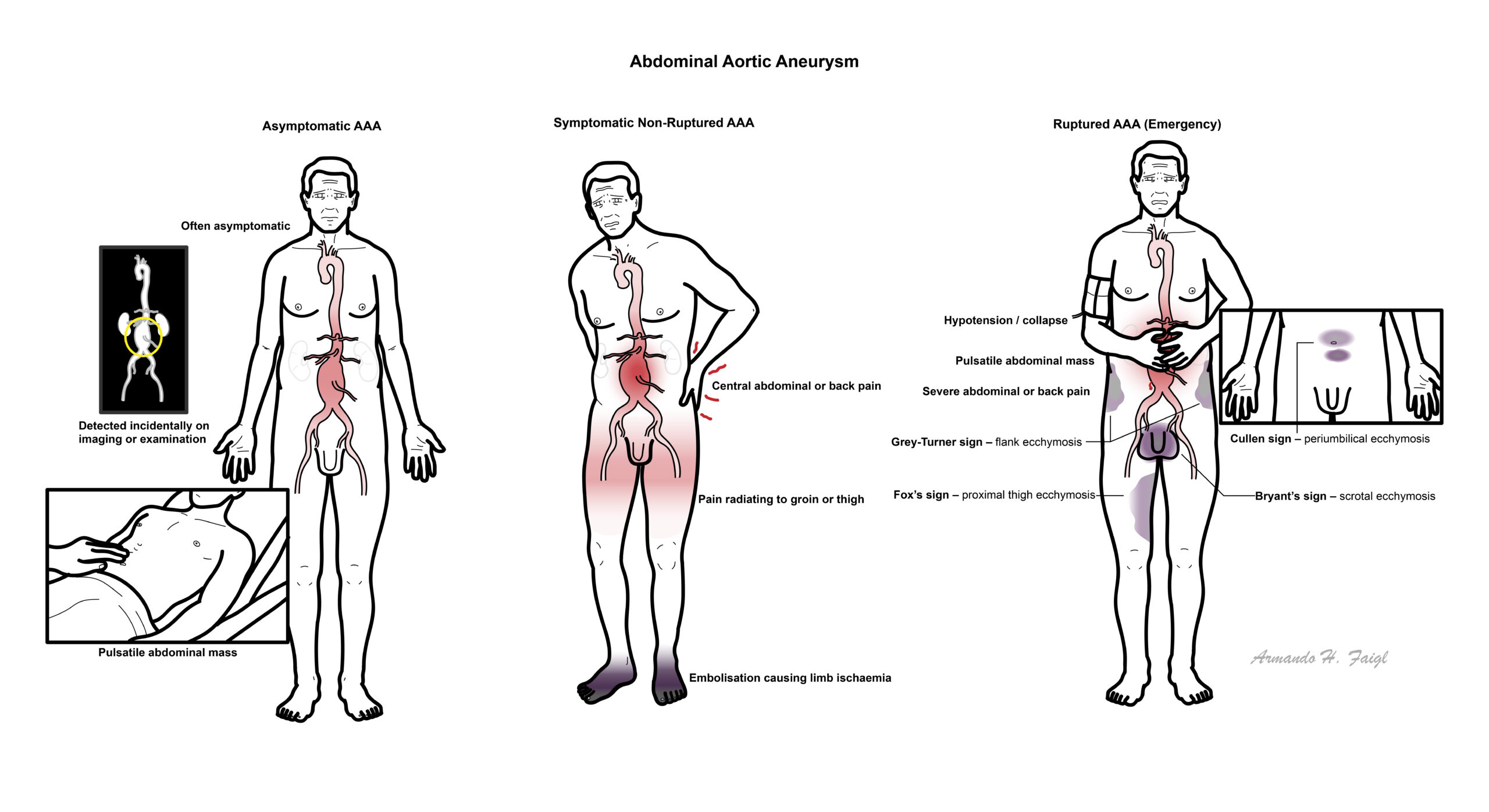
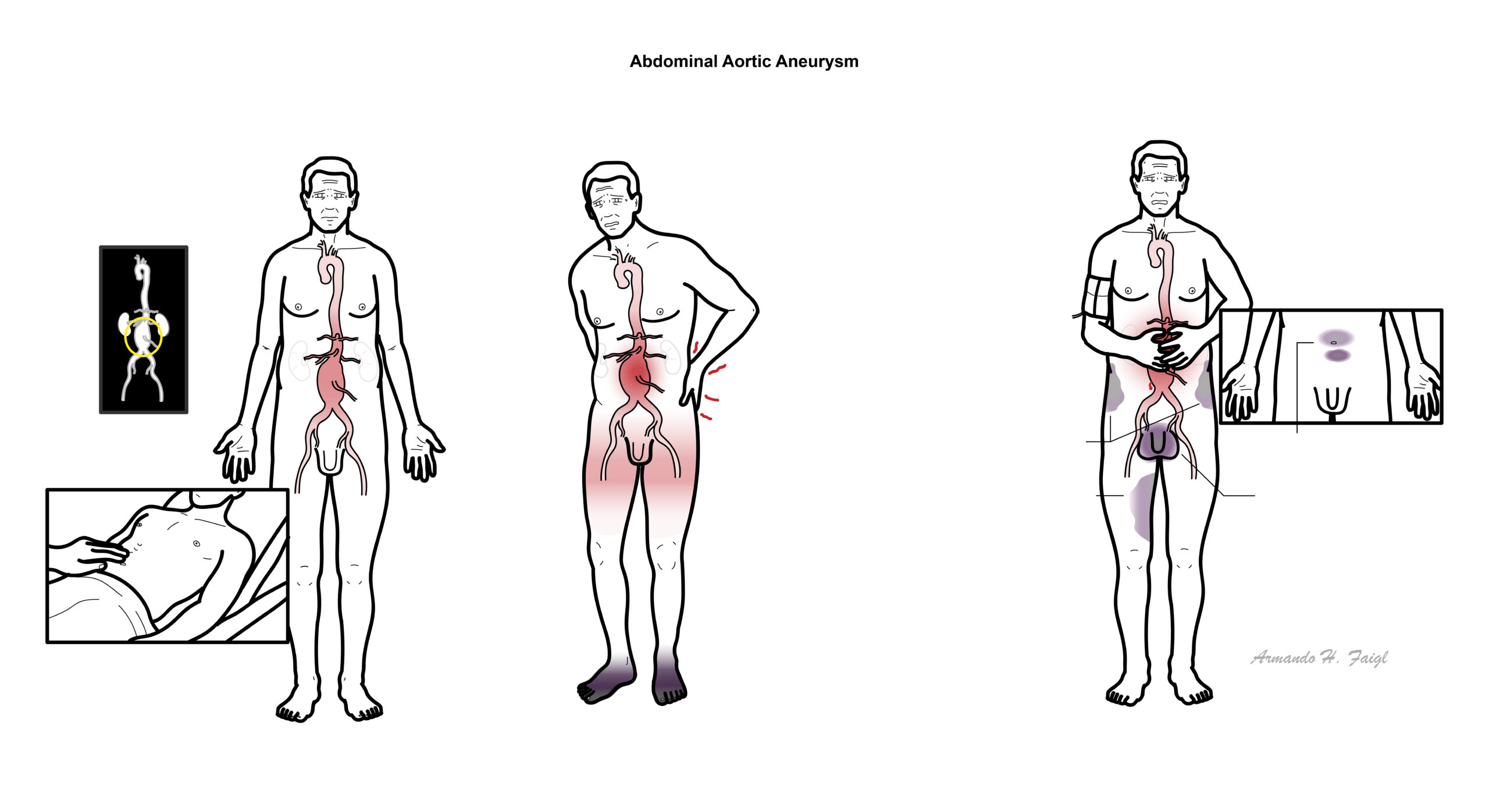
Clinical Manifestation
Asymptomatic AAA:
- Incidental finding or on routine physical examination, AXR or abdominal ultrasound
- May have a pulsatile abdominal mass on palpation
- Consider for treatment or surveillance
Symptomatic non-ruptured AAA:
- Pain in central abdomen, back, flank, pelvis, thigh or groin
- Thrombus in aneurysmal sac may be a source of emboli to lower limbs causing limb ischaemia
- Compression of surrounding structures and accompanying symptoms – left ureter, duodenum, lumbar nerve roots, IVC
Ruptured AAA – triad:
- Back/Abdominal pain
- Hypotension/collapse
- Pulsatile abdominal mass 1 4
Examination
- Abdominal palpation: pulsatile abdominal mass
- Vascular examination – if limb ischaemia suspected
- Ecchymosis – may be present if AAA ruptures (indicates extensive retroperitoneal haematoma); method of description based on location:
- Grey-Turner sign: flank ecchymosis
- Cullen sign: periumbilical ecchymosis
- Fox’s sign: proximal thigh ecchymosis
- Bryant’s sign: scrotum ecchymosis 4
Diagnosis
- Acute Pancreatitis
- Mesenteric Ischaemia
- Ruptured gastrointestinal ulcer
- Appendicitis
- Gallstone Disease
- Nephrolithiasis
- Irritable Bowel Syndrome
Investigation
Aortic ultrasound – used for screening asymptomatic patients and symptomatic patients who are haemodynamically unstable; cannot definitively rule out ruptured AAA
CT angiogram – used for pre-op planning and patients with symptomatic AAA who are haemodynamically stable
Patients with known history of AAA and symptoms of rupture can be diagnosed based on clinical examination alone 1 4
Do not delay diagnosis and management of a ruptured AAA while waiting for imaging results.
Classic triad of ruptured AAA: hypotension/collapse, back/abdominal pain, palpable/pulsatile mass.
- Acute pancreatitis
- Mesenteric Ischaemia
- Perforated peptic ulcer
- Diverticulitis
- Appendicitis
- Renal colic (nephrolithiasis)
- Irritable Bowel Syndrome
- Inflammatory Bowel Disease
Treatment
Asymptomatic AAA:
- Cardiovascular risk reduction: smoking cessation, controlling hypertension, hyperlipidaemia, diabetes, clotting risk
- Surveillance – aortic ultrasound
- Elective surgical repair 5
| AAA diameter (cm) | Surveillance interval |
| >2.5 but <3.0 | 10 years |
| 3.0 – 3.9 | 3 years |
| 4.0 – 4.9 | 12 months |
| 5.0 – 5.4 | 6 months |
Indications for AAA repair:
- Male with AAA of 5.5 cm or above
- Female with AAA >5.0 cm
- Aneurysm >4cm and rapid growth >1.0 cm per year
- Symptomatic AAA 1 5
Risk of rupture based on aortic diameter: 6
| Baseline aortic diameter (cm) | 12-month rupture risk |
| 3.0 – 3.9 | <1% |
| 4.0 – 4.9 | 1% |
| 5.0 – 5.9 | 1.7 – 11% |
| 6.0 – 7.0 | 5.1 – 22% |
| >7.0 | 19 – 33% |
Ruptured and symptomatic non-ruptured AAA – urgent surgical management:
- Emergency Endovascular Aneurysm Repair (EVAR) – placement of graft via the femoral arteries, lining the aorta and excluding the aneurysm sac; recommended in most patients
- Open repair – replacement of diseased aortic segment with a tube or bifurcated prosthetic graft via an abdominal incision; recommended for younger patients with connective tissue disorders 1 7
Ruptured AAA resuscitation – restrictive resuscitation with blood products aiming for permissive hypotension – prevents worsening of bleed: higher BP would lead to higher pressure on aortic wall and disruption of temporary clot, and increase in fluid level may cause dilutional coagulopathy.
Rupture into the peritoneal cavity is usually rapidly fatal due to blood having more space to spread. In a retroperitoneal rupture, the blood has limited space to spread and bleeding is reduced, which may cause the rupture to transiently stabilise, providing a window of opportunity for lifesaving intervention.
Complications
Complications of AAA:
- Death
- Rupture
- Myocardial infarction
- Renal failure
- Lower limb embolism
- Gut ischaemia
- Abdominal compartment syndrome
- Fistula formation (eg. aorto-enteric)
Repair-related complications:
- Endoleaks
- Graft migration
- Graft infection
- Organ ischaemia
References
- McMahon G. Abdominal aortic aneurysm. In: BMJ Best Practice [Internet]. 2025 [cited 2026 Feb 8]. Available from: BMJ Best Practice
- Wilkinson IB, Raine T, Wiles K, Hateley P, Kelly D, McGurgan I, et al. Surgery. Oxford Handbook of Clinical Medicine: Oxford University Press; 2024. Available from: https://doi.org/10.1093/med/9780198844013.003.0013
- Dalman RL, Mell M. Overview of abdominal aortic aneurysm. In: Collins KA, editor. [Internet]. [updated 2025 May 14; cited 2026 Feb 8]. Available from: UpToDate
- Jim J. Clinical features and diagnosis of abdominal aortic aneurysm. In: Collins KA, editor. [Internet]. [updated 2024 Jul 19; cited 2026 Feb 8]. Available from: UpToDate
- Dalman RL, Mell M. Management of asymptomatic abdominal aortic aneurysm. In: Collins KA, editor. [Internet]. [updated 2025 Sep 26; cited 2026 Feb 8]. Available from: UpToDate
- Chung J. Epidemiology, risk factors, pathogenesis, and natural history of abdominal aortic aneurysm. In: Collins KA, editor. [Internet]. [updated 2024 May 10; cited 2026 Feb 8]. Available from: UpToDate
- Jim J. Management of symptomatic (non-ruptured) and ruptured abdominal aortic aneurysm. In: Collins KA, editor. [Internet]. [updated 2024 Sep 3; cited 2026 Feb 8]. Available from: UpToDate




Members only discussions coming soon…