

Temporal Arteritis (Giant Cell Arteritis)

Overview
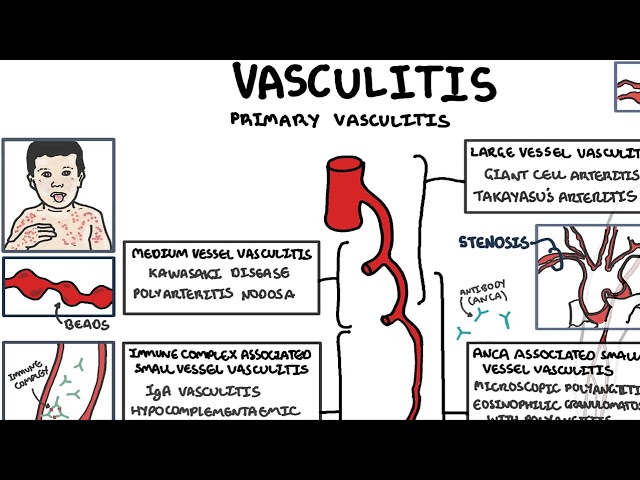
Giant cell arteritis affects medium and large arteries and can result in blindness. Giant Cell arteritis is common in the elderly. Consider Takayasu’s arteritis if under 55yo. It is associated with polymyalgia rheumatica in 50% of cases.
Giant cell arteritis, the most common type of vasculitis in adults, affects medium and large arteries and can result in blindness.
Giant cell arteritis does not always involve the temporal artery and can affect other medium and large arteries including the aorta.
Definition
Giant cell arteritis: Systemic inflammatory vasculitis of unknown aetiology that occurs in older persons
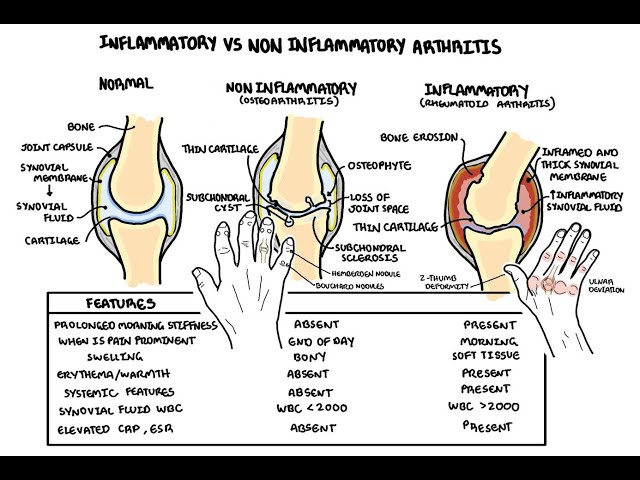
Polymyalgia rheumatica: Commonest inflammatory rheumatic disorder affecting older people. Patients typically present with bilateral shoulder pain, morning stiffness, raised inflammatory markers, and have a rapid response to low-dose corticosteroids
Takayasu’s arteritis: chronic granulomatous vasculitis affecting large arteries: primarily the aorta and its main branches.
Clinical Manifestation
Clinical Presentation
- Headache (85%)
- Jaw or tongue claudication, defined as pain or weakness in the muscles of mastication that begins just after the onset of chewing and is relieved by rest, occurs with giant cell arteritis
- Fatigue
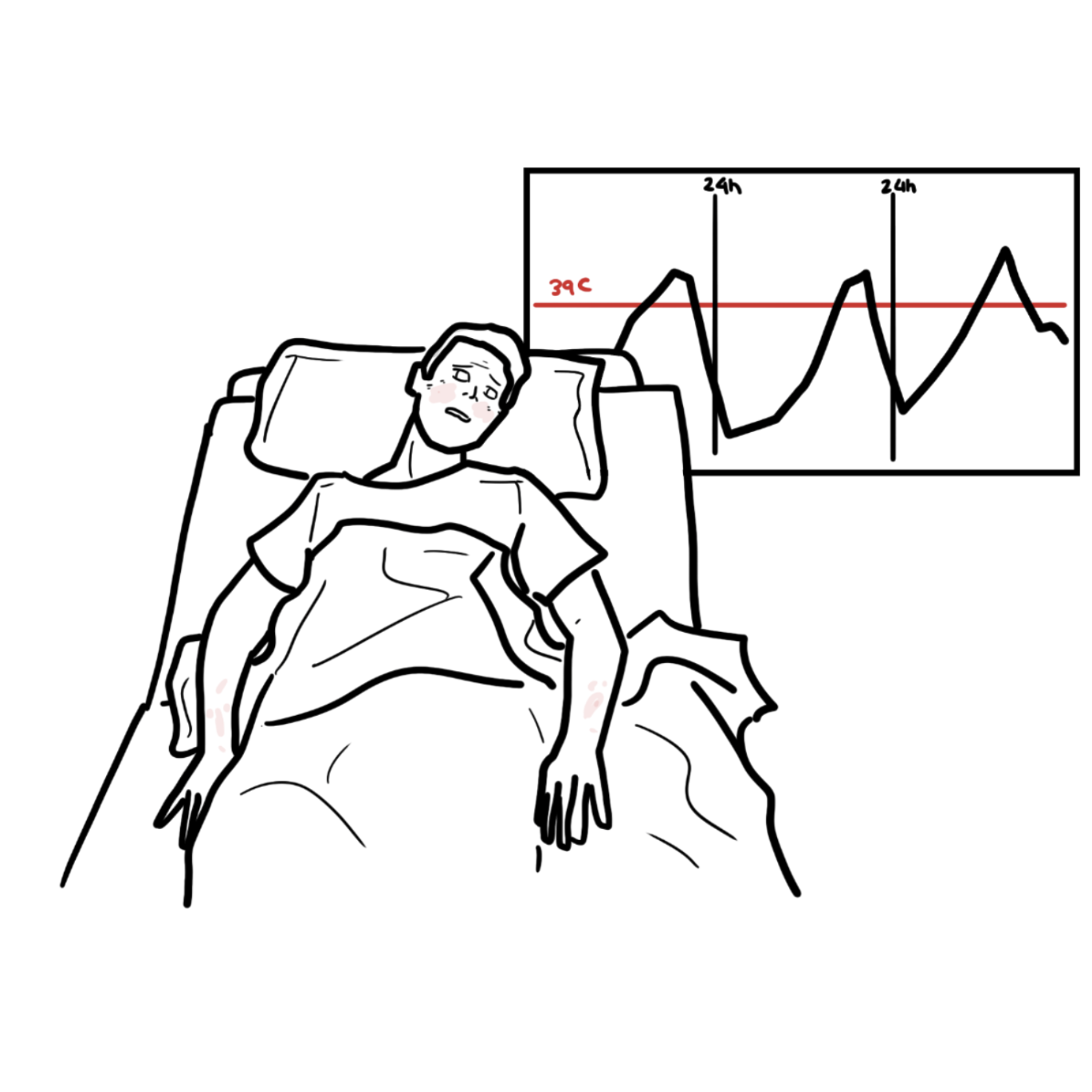
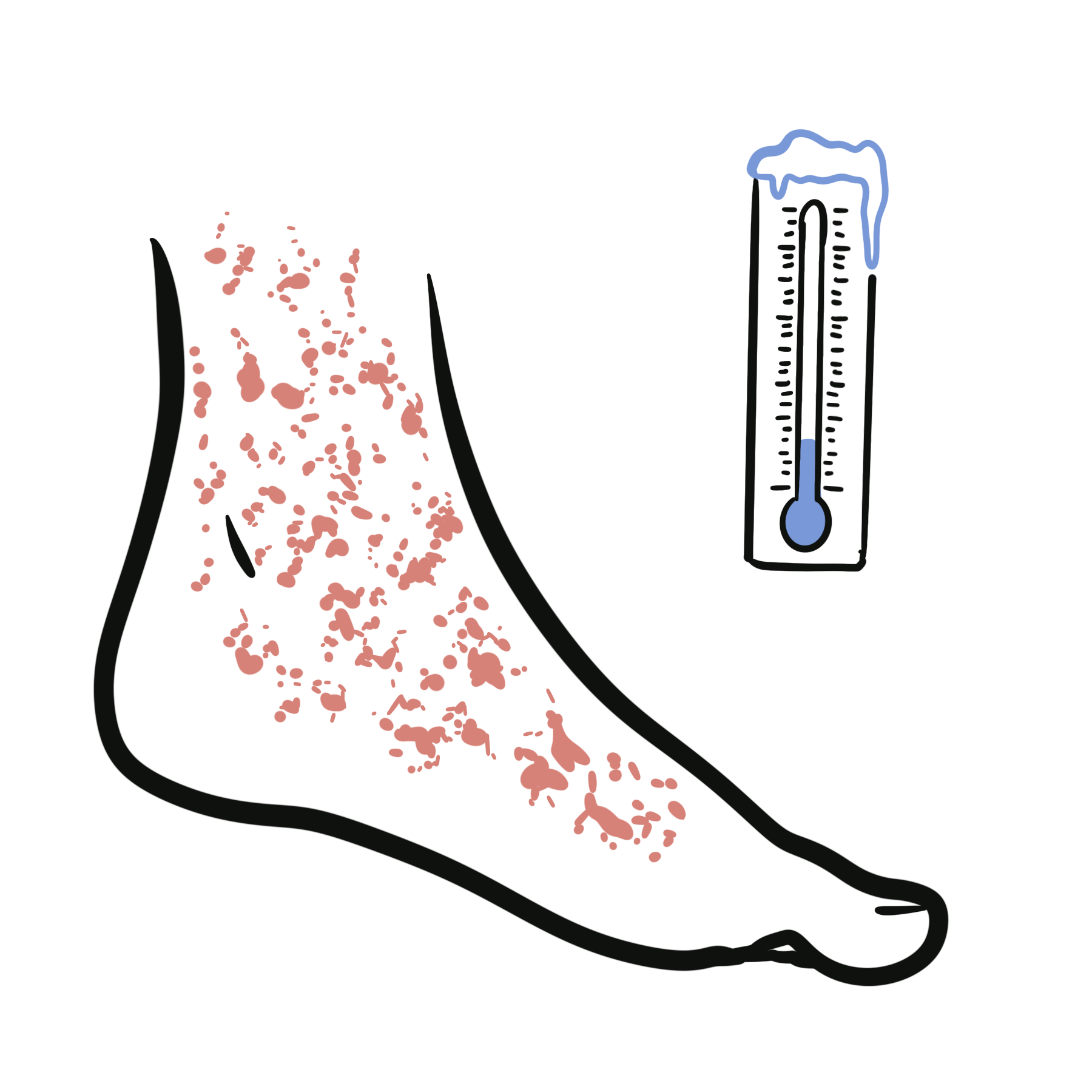
- Fever
- Weight loss
- Anorexia
- Polymyalgia rheumatica (50% of cases)
- Visual disturbance
- Visual loss
- Peripheral neuropathy
- Cough
Jaw claudication and visual symptoms are ischemic warning signs.
Polymyalgia rheumatica Commonest inflammatory rheumatic disorder affecting older people. Patients typically present with bilateral shoulder pain, morning stiffness, raised inflammatory markers, and have a rapid response to low-dose corticosteroids.
Diagnosis
- Infections
- Malignancy (especially myelodysplasia)
- ESR
- CRP
- Vascular imaging
- Temporal artery biopsy
- Ultrasound of temporal artery ‘halo sign’
- Age >50 years (peaks 75yo)
- New onset of localised headache
- ESR ≥50 mm/hr
- Temporal artery tenderness or decreased temporal artery pulse
- Positive temporal artery biopsy
Imperative to obtain adequate temporal artery biopsy (>2cm) because GCA presents as skip lesions.
ESR maybe normal initially.
Treatment
- Prednisolone high dose
- Antiplatelet therapy – decreases cranial ishcaemic complications
- Proton pump inhibitors
- Bisphosphanates, calcium and Vitamin D – bone protection
- Review
If you suspect GCA do ESR and start prednisolone immediately without waiting biopsy results!
Complications and Prognosis
- Typically a 2 year course, then complete remission.
- Decrease steroid dose when symptoms go, increase if ESR increases
GCA and PMR are among the most common inflammatory rheumatic diseases in the elderly; the prevalence of these diseases is expected to increase due to ageing of the population.







Members only discussions coming soon…