

Chagas Disease

Authors
Megan Miner
Armando Faigl
Overview
Chagas disease is caused by the parasitic protozoan Trypanosoma cruzi (T. cruzi) and is potentially life-threatening. These parasites often live within triatomine bugs. Following a bite to the skin, these bugs, also known as “kissing bugs”, deposit fecal matter near the site of the bite. Their bite, unfortunately, causes the person to scratch, thus allowing the fecal matter (and T. cruzi parasite) to enter systemic circulation, thus, causing the disease. There are two stages to Chagas disease, acute and chronic.
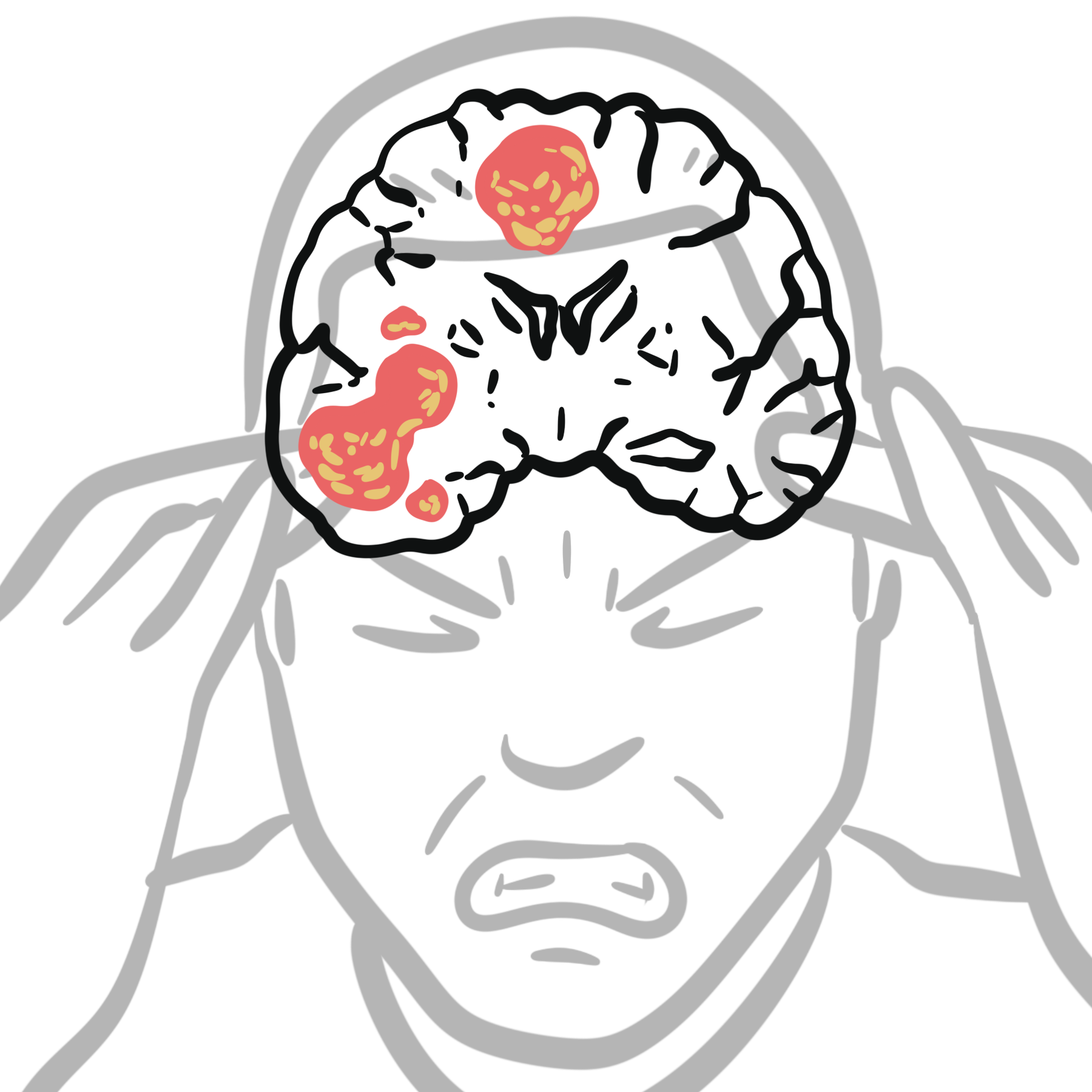
Triad for chronic Chagas disease: cardiomegaly, enteromegaly, and neurological symptoms.
Definition
Chagas Disease: Disease resulting from the T. cruzi parasite.
Trypanosoma cruzi: A parasitic protozoan that lives, typically, in the triatomine bug
Triatomines: An insect that carries the T. cruzi parasite
Aetiology & Risk Factors
- Low socioeconomic status (triatomines live in walls and ceilings that are made from mud or straw)
- Geographical location (Mexico, Central America, and South America)
- Poor hygiene.
Life Cycle of Trypanosoma cruzi
- The parasites multiply in the midgut of the triatomine bugs (kissing bug) as promastigotes.
- In the hindgut, they transform into trypomastigotes which pass out in the faeces during blood meals.
- The faecal matter containing parasite invade humans from skin breaks
- The parasites enter host cells, transform into amastigotes, and multiply and differentiate into trypomastigotes.
- The cell ruptures, releasing the parasites which invade local tissue and spread hematogenously
Pathophysiology
Chagas disease and its associated symptoms are caused by the T. cruzi parasite and is transmitted to humans via triatomine bugs.
Other routes of transmission:
- Vertical transmission
- Blood transfusion
- Organ transplantation
- Oral transmission (contaminated food)
- Laboratory exposure.
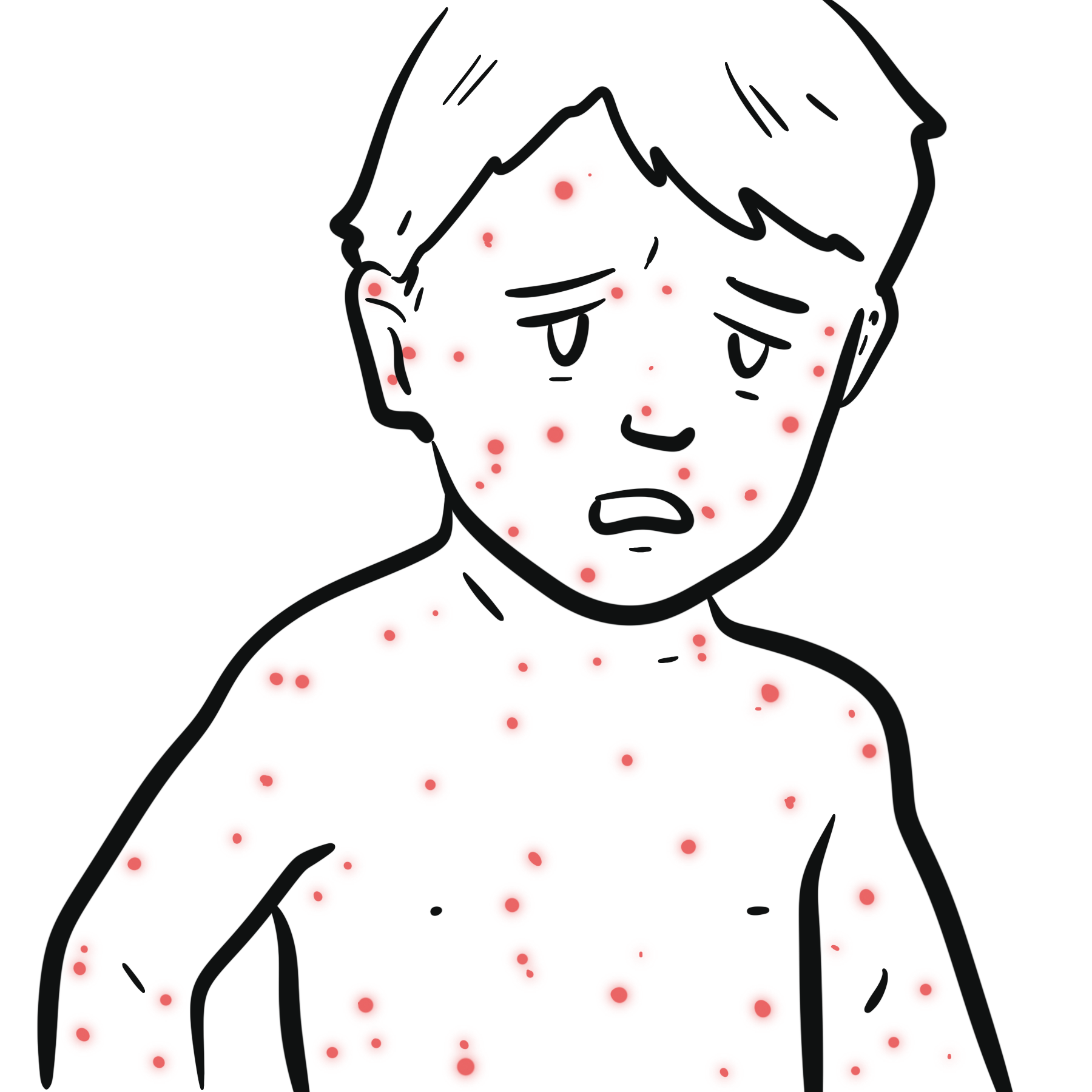
Acute Chagas’ disease is usually an illness of children. During the acute phase, many may display viral symptoms. An inflammatory lesion called a chagoma develops at the site of entry. Romana’s sign (painless periorbital oedema) may be seen if the site of entry is the conjunctiva.
Innate immunity increases cytokine and chemokine production in response to the parasitic infection. The adaptive immune system produces B cells, T cells, and antibodies. Gradually, parasite levels drop, and the patient enters an asymptomatic phase. The person now enters the intermediate phase. There is no sign of the parasite, except for IgG produced against T. cruzi.
Severe myocarditis with CCF may occur in the acute phase.
After the acute phase patients enter the asymptomatic phase. There is no sign of the parasite, except for IgG produced against T. cruzi. Years later chronic chagas disease can reemerge.
Chronic Phase of infection
About 30% of people will develop the chronic phase of Chagas disease 15-30 years after being bitten. The main organs affected is the heart or the gastrointestinal tract.
Chronic phase: Cardiac Disease
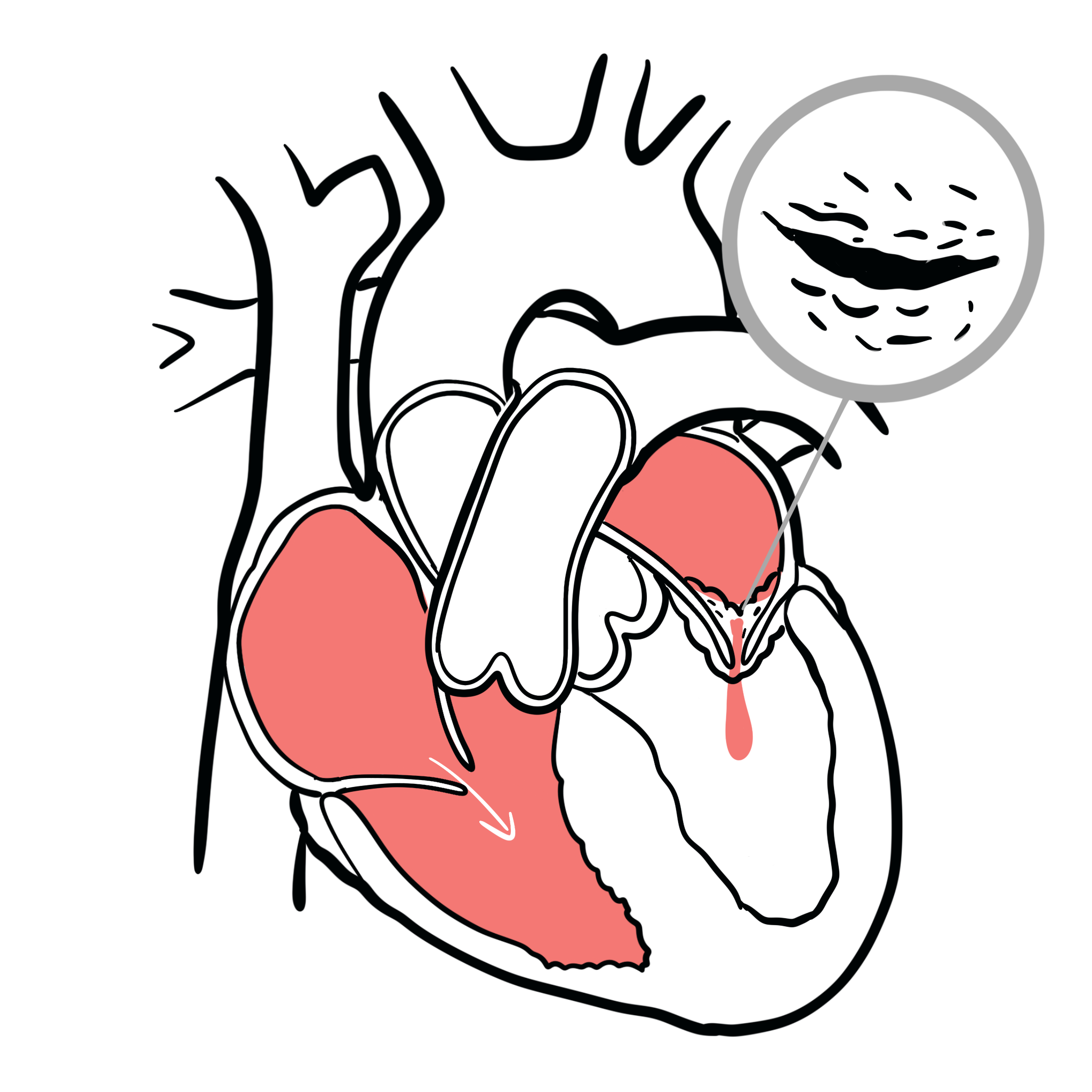
Specifically in the heart, Chagas disease results in:
- Dilated cardiomyopathy (figure 1)
- Cardiac failure
- Arrhythmias
- Pulmonary and systemic emboli, and stroke.
Chronic phase: Gastrointestinal Disease
- Common organ system affected in chronic Chagas disease, again muscle cells here are affected leading to enteromegaly
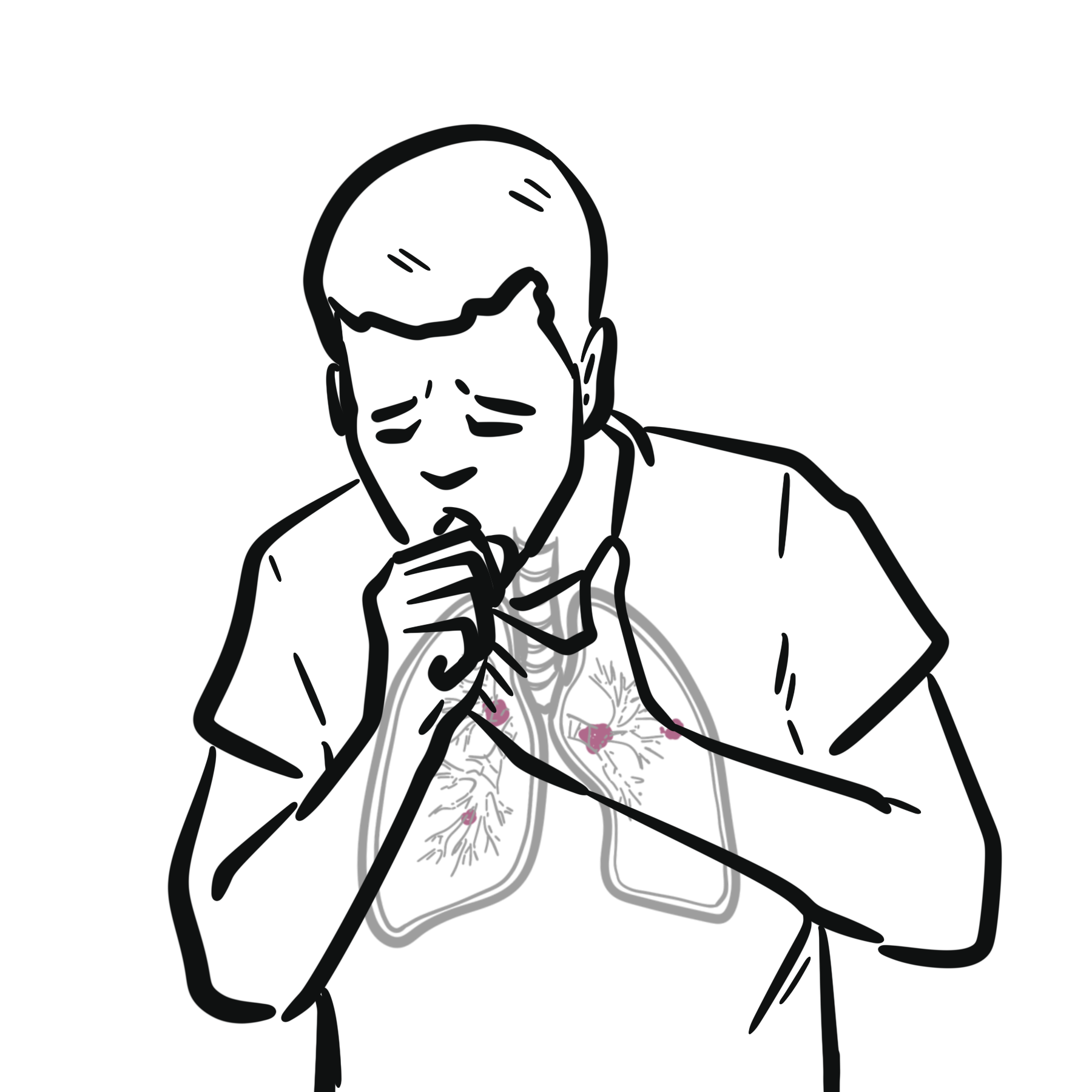
- Achalasia and megaoesophagus
- Regurgitation and dysphagia can lead to aspiration pneumonitis which is common and may be fatal.
- Megacolon
- Achalasia and megaoesophagus
- ↑oesophageal cancer
Clinical Manifestation
Acute Phase
- Romaña’s sign (painless periorbital oedema) may be seen if the site of entry is the conjunctivae
- Fever
- malaise, anorexia
- anorexia
- oedema
- lymphadenopathy
- Hepatosplenomegaly
- Myocarditis (rare)
Chronic Phase related to organ complications
- Cardiomegaly
- Congestive heart failure (CHF)
- Arrhythmias
- Cardiac arrest
- Enteromegaly – achalasia, megaoesophagus, megacolon
Diagnosis
- Esophageal motility disorders
- Gastroesophageal reflux disease (GERD)
- Malaria
- Meningitis
- Myocardial infarction (MI)
- Coronary artery disease (CAD)
- Esophageal rupture
- Angina pectoris
- Hirschsprung Disease
- Constipation
Investigations
Acute Phase
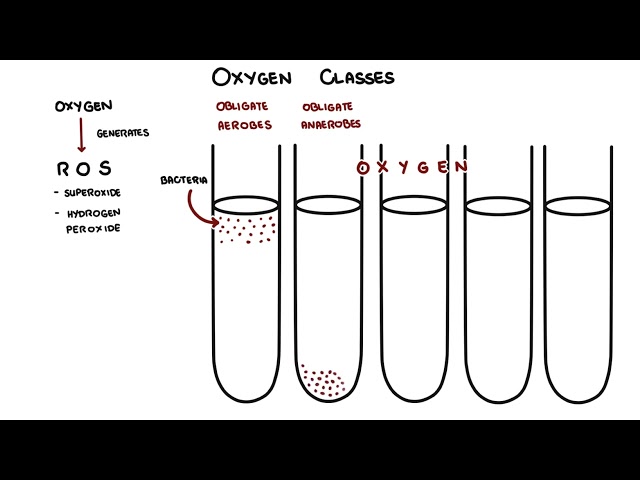
- Blood film
- wet prep or Giemsa smear for detection of circulating parasites, Trypomastigotes
- Blood culture
Chronic Phase
- In order to diagnosis a chronic Chagas disease, a mixture of clinical findings and the patient’s likelihood that they would have been infected are discussed
- IgG antibodies to the parasite
- If chronic Chagas disease is likely, then the following tests are advised:
- Electrocardiogram (ECG) – RBBB, heart block
- Chest and abdominal X-ray
- Cardiac Echo
- Gastroscopy and colonscopy
Chronic Chagas’ disease is diagnosed by detection of IgG antibodies to the parasite in the presence of clinical symptoms.
Classification
Acute Phase
- Lasts approximately two months
- Symptoms may start 1-2 weeks after bite
- Romana’s sign (painless periorbital oedema)
- Fever, fatigue, body aches, rash, diarrhea, or vomiting
Chronic Phase
- Upwards of 80% of people are asymptomatic
- 20-30% will progress
- Cardiovascular and or gastrointestinal disease
- Cardiomegaly, arrhythmias, enteromegaly,
- Symptoms don’t appear again until 15-30 years after initial infection period
- Cardiovascular and or gastrointestinal disease
Treatment
Acute Phase Chagas Disease
- Benznidazole (nitroimidazole antimicrobial)
- Contraindicated for those with history of psychiatric disorders, pregnancy, severe renal and liver dysfunction and alcohol misuse
- Side effects include rash, peripheral neuropathy, and bone marrow suppression
- Nifurtimox
- Contraindicated for those with history of psychiatric disorders, pregnancy, severe renal and liver dysfunction
- Side effects include nausea, vomiting, abdominal pain, weight loss, and neurological symptoms
Chronic infection
- treatment is supportive.
- Pacemakers are helpful in patients with bradyarrhythmias.
- Megaoesophagus may be treated with balloon dilatation/myomectomy of the lower oesophageal sphincter.
- Megacolon is managed with high-fibre diet and laxatives/enemas. Surgery may be required for complications.
Complications & Prognosis
Complications
- Cardiac arrhythmia
- Heart failure
- Infections to the brain or heart
- Cardiomegaly
- Scarring
- Cardiomyopathy
- Myocarditis
- Enteromegaly
Patients with chronic Chagas disease (including those with cardiomyopathy) have a poor prognosis. However, many live with the disease unbeknownst to them. Likewise, early intervention with medication provides patients with an optimistic prognosis.








Members only discussions coming soon…