Pertussis


Author
Megan Miner
Armando Faigl
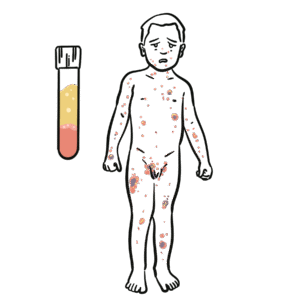
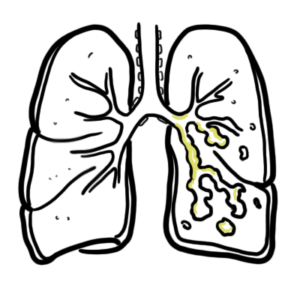
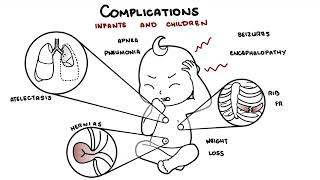
Pertussis, also known as “whooping cough”, is a contagious, acute respiratory infection caused by the bacterium Bordetella pertussis. In babies, the infection can sometimes lead to pneumonia and occasionally brain damage and can even be life threatening. Older children and adults can get whooping cough and can spread it to others, including babies. Pertussis causes its severe symptoms via the release of deleterious proteins such as; filamentous hemagglutinin, pertactin, agglutinin, tracheal cytotoxin, pertussis toxin, and adenylate cyclase toxin.
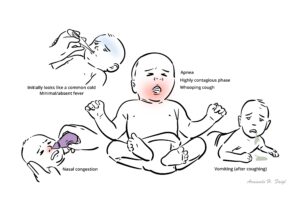
Triad: afebrile respiratory infection, a whooping cough (with increasing frequency and severity) and coryza.
Bordetella pertussis: Bacterium that causes an acute respiratory infection which results in a severe “whooping” cough as a consequence of the release of noxious proteins as described above.
Bordetella parapertussis: Bacterium that causes pertussis-like-illness without the release of pertussis toxin. A “whooping” cough may or may not be present.
Filamentous hemagglutinin (FHA): Protein expressed and secreted by Bordetella pertussis in order to anchor to cilia and attach to host immune cells (macrophages).
Pertactin: Protein used by the bacterium in order to anchor to cilia.
Agglutinin: Protein used by the bacterium in order to anchor to cilia
Tracheal cytotoxin: Paralyzes and kills cilia, allowing the bacterium and mucus to stay “stuck” in the respiratory tract [3]. This elicits a cough reflex.
Pertussis toxin: Helps anchor Bordetella pertussis to respiratory epithelium and triggers an increased T cell production. Also makes the respiratory system more responsive to histamine [3] which causes swelling to the airway and the classic “whooping cough”.
Adenylate cyclase toxin: Prevents phagocytes from reaching the infection and induces apoptosis in such cells.
Bacterium Bordetella pertussis which is easily spread via aerosolized droplets (cough/sneeze etc), especially during the Catarrhal phase.
Bordetella Pertussis is a gram negative coccobacilli.
Incubation (disease develops in 1-2 weeks)
Following incubation there are three stages of the illness. Please note adolescents and adults often don’t present with the classic pertussis syndrome below seen in young children.
Catarrhal Phase (occurs after incubation and lasts roughly 1-2 weeks)
It is best to diagnose pertussis during this phase to reduce mortality and prevent severe damage
Paroxysmal Phase (occurs after Catarrhal phase and lasts roughly 1-6 weeks)
Convalescent Phase (occurs after Paroxysmal phase and lasts roughly 2-3 weeks)
Culture of nasopharyngeal secretions is considered gold standard for diagnosing pertussis.
Pertussis is contagious do not go near babies or pregnant women.
Treatment with macrolides in infants less than 1 month old should be used with caution due to the association with the development of infantile hypertrophic pyloric stenosis.
Complications in Infants and Children
Complications in Adolescents and Adults
Those diagnosed with pertussis that are over the age of three months are typically expected to make a full recovery. Those under the age of three months may be associated with more severe symptoms, however mortality rates are less than 3%.
Prognosis is generally grimmer for those that are at-risk (unvaccinated, immunocompromised, or infant/elderly populations).











Discussion