

Hydrocephalus
Overview
Hydrocephalus is excessive accumulation of CSF in the cerebral ventricles. In children, look for increasing head circumference, increased intracranial pressure, a bulging fontanelle, scalp vein engorgement, and paralysis of upward gaze. The most common causes include:
- Congenital malformations
- Tumors
- Inflammation (i.e hemorrhage, meningitis).
Treat the underlying cause, if possible; otherwise a surgical shunt is created to decompress the ventricles.
Anatomy & Physiology of CSF
- CSF is produced primarily by the choroid plexus, which is responsible for 60 to 80 percent of CSF production.
- The choroid plexus tissue is located in each cerebral ventricle and consists of villous folds lined by epithelium with a central core of highly vascularized connective tissue.
- CSF supplies brain tissue with nutrients and flows through the ventricles before being absorbed back into circulation from the venous sinus.
- CSF production rates are constant in physiological conditions unless extremely high levels of intracranial pressure are reached.
- Thus, absorption of CSF generally matches the rate of production to accommodate the volume of CSF being formed each day.
- CSF returns to circulation via the venous sinus.
Aetiology & Risk Factors
| Infantile Risk Factors |
| Birth weight <1500 g |
| Prematurity (gestational age ≤30 weeks) |
| Maternal diabetes |
| Low socioeconomic status |
| Male sex |
| Race/ethnicity (the risk is decreased in Asians) |
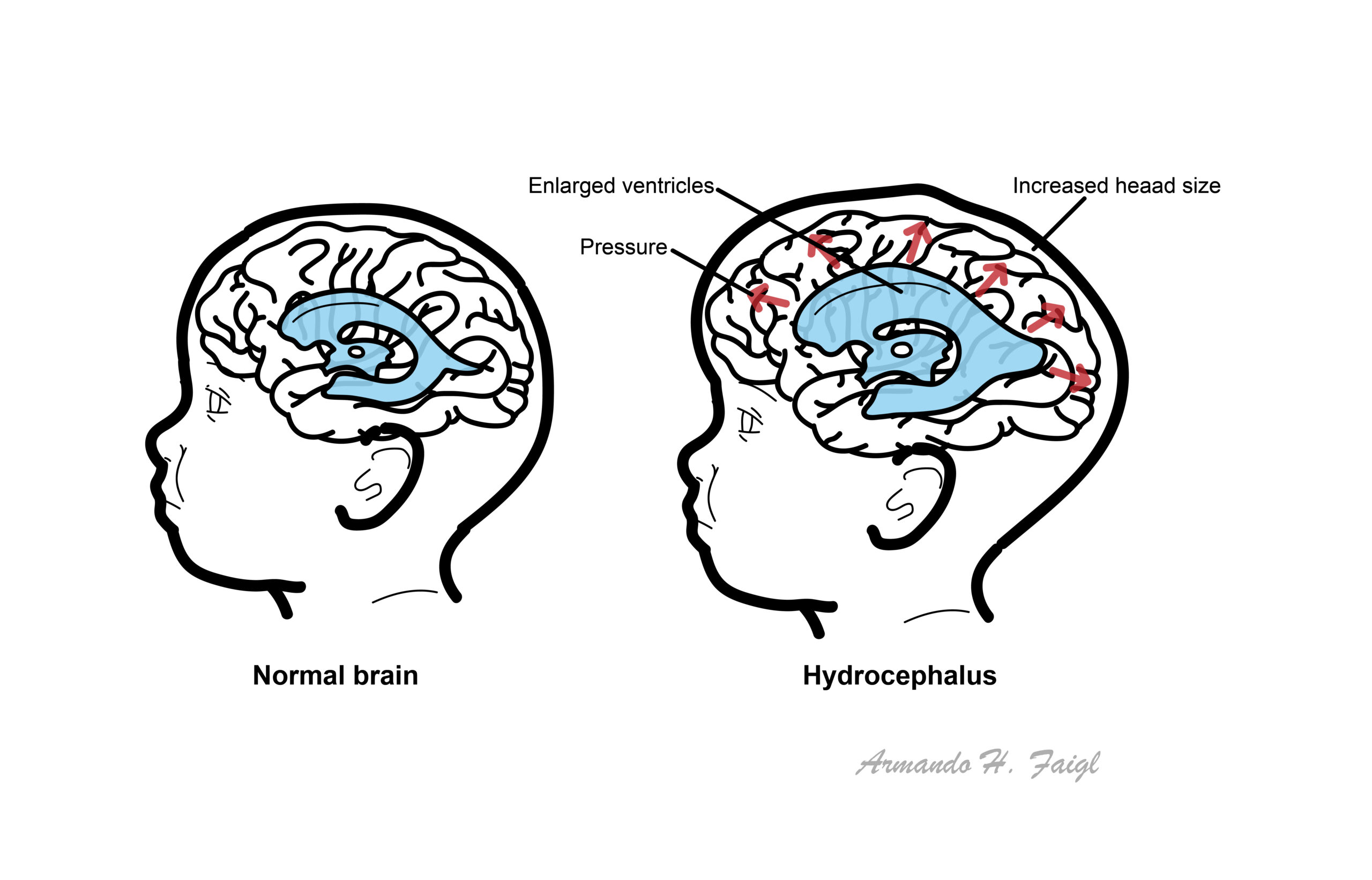
Pathophysiology
Excessive accumulation of cerebrospinal fluid in the brain that can be due to:
- Increased production of CSF (rare)
- CSF flow obstruction (most common) also known as non-communicating
- Decreased absorption of CSF also known as communicating
Many cases of hydrocephalus have both obstructive and absorptive components.
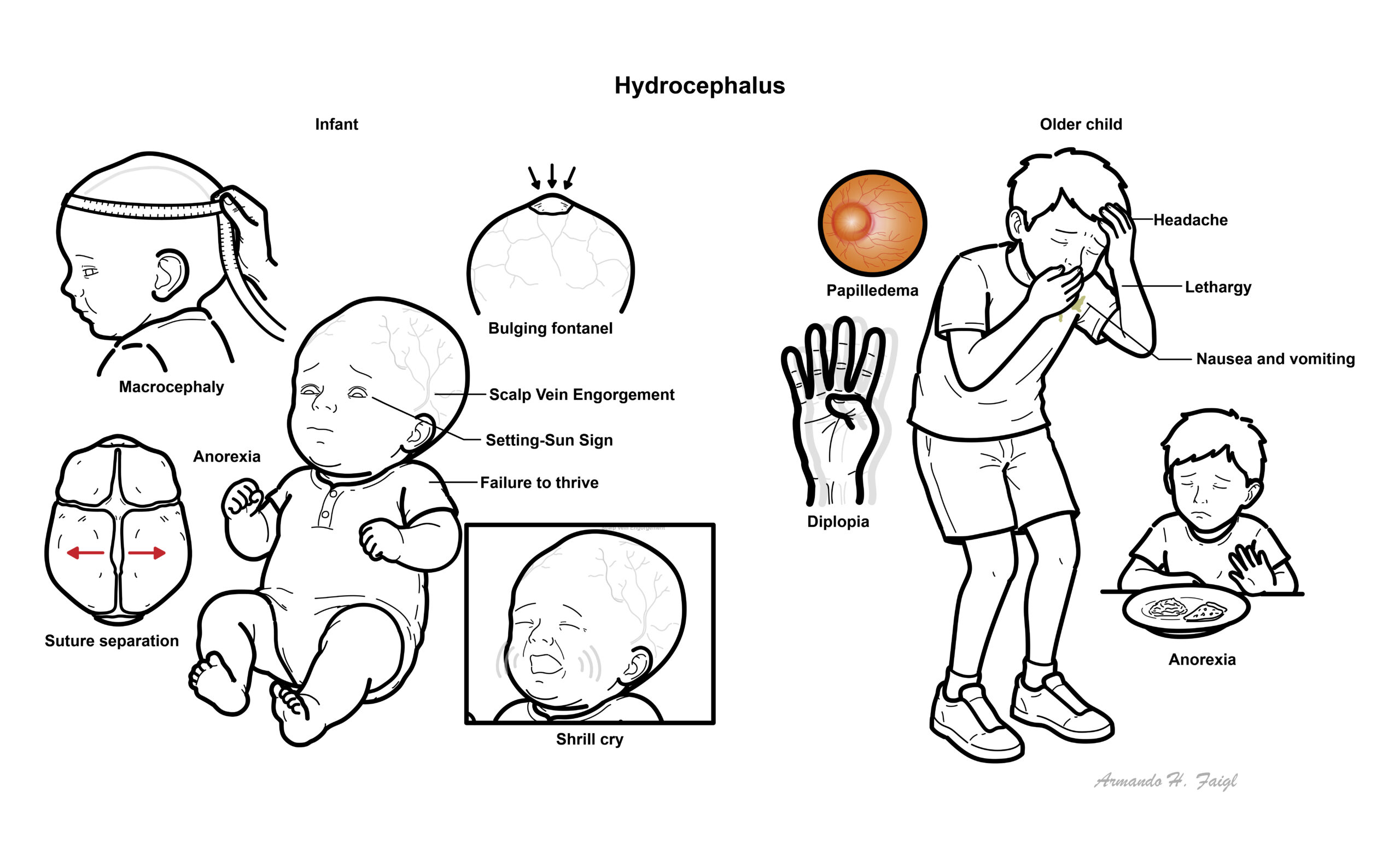
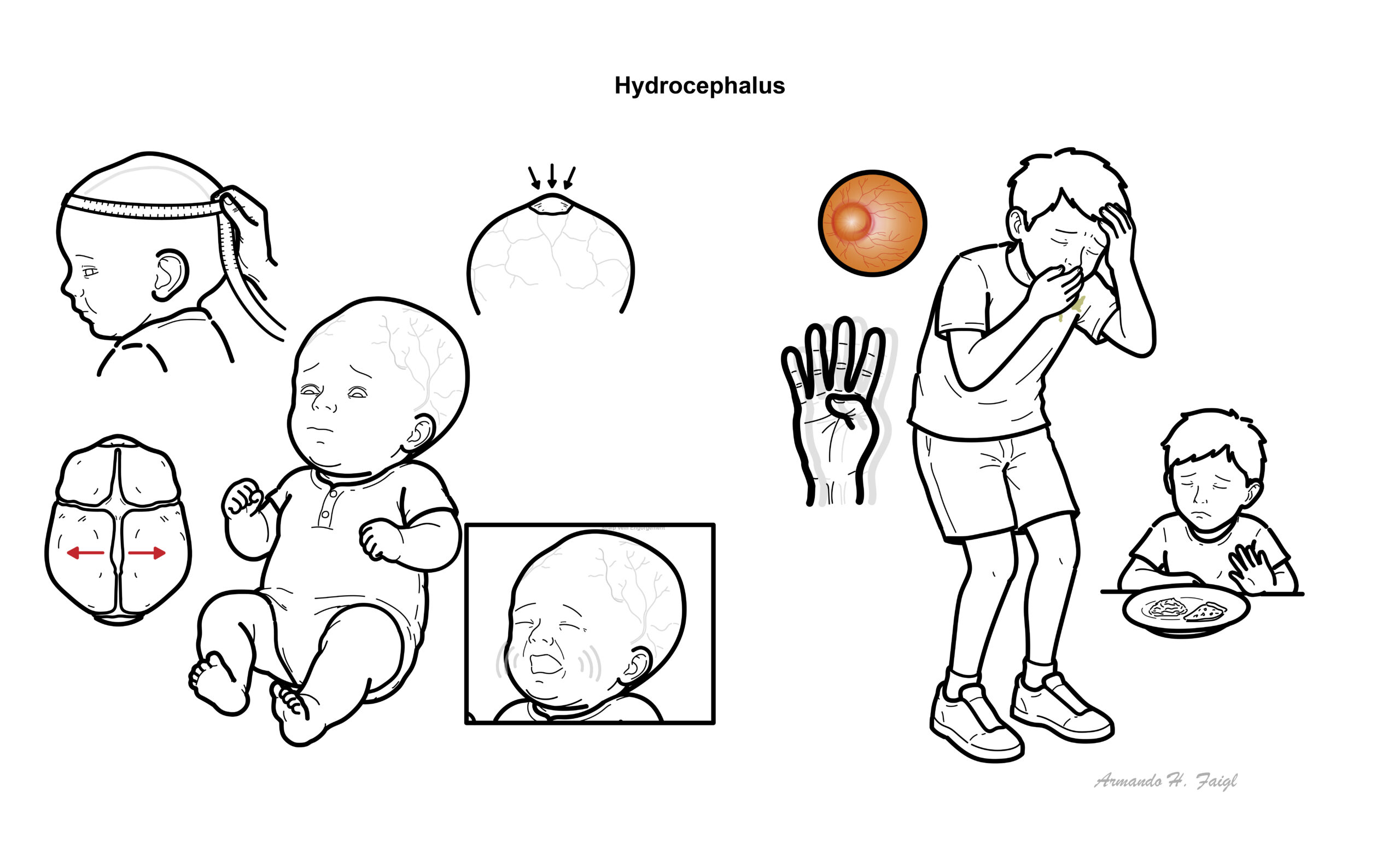
Clinical Manifestation
| DIFFERENT BETWEEN INFANT AND OLDER CHILDREN | |
| Infant | Older Child |
| Increasing head circumference, Macrocephaly | Headache (morning worse) |
| Delayed closure of the fontanel | Nausea and vomiting |
| Suture separation | Personality and mood changes |
| Bulging fontanel | Lethargy |
| Failure to thrive | Anorexia |
| Paresis of upward gaze (known as setting-sun sign) | Diplopia as a result of sixth-nerve palsy or third-nerve palsy with uncal herniation |
| Shrill cry | Papilledema |
Diagnosis
- Neurofibromatosis
- Pituitary gigantism
- Sotos syndrome
- Achondroplasia
Hydrocephalus should be suspected in an infant whose head circumference is enlarged at birth or in whom serial measurements cross percentiles in standard growth curves, indicating excessive head growth. Hydrocephalus should be considered in children with severe headache and other features suggesting increased intracranial pressure (ICP).
- Serial Head circumference
- Head ultrasound
- CT
- MRI
- Pressure flow studies
In a newborn, ultrasonography is the preferred technique for the initial examination because it is portable and avoids ionizing radiation. As the anterior fontanelle closes, the ultrasound is no longer a useful diagnostic modality.
In older infants and children with suspected hydrocephalus, CT or MRI should be performed. These imaging studies will also detect associated central nervous system (CNS) malformations or tumors.Brain imaging can help to distinguish obstructive (non-communicating) from absorptive (communicating) hydrocephalus.
- Head circumference increases at an abnormal rate, passing 2 deviation
- The diagnosis of hydrocephalus is confirmed by neuroimaging.
Classification
Hydrocephalus can be divided up into congenital and acquired
Congenital Hydrocephalus are picked up on ultrasound
- In uterus infections
- Aquedcut stenosis
- Dandy walker malformation
- Chiari malformation (associated spina bifida)
Acquired Hydrocephalus – usually occur later in life due to some sort of “event”
- Meningitis
- Haemorrhage (bleeding)
- Tumours
Hydrocephalus can be communicating or non-communicating
- Communicating – ventricles are connect without obstruction
- Non-communicating – ventricles are not connected because of an obstruction
Hydrocephalus ex vacuo describes increases in CSF volume without increased CSF pressure, which is seen in conditions of reduced cerebral tissue (i.e malformation, atrophy).
Treatment
- Transfer as an emergency -> neurosurgery clinic for review
- Ventricular tap
- Shunt
- Ventricuoatrial
- Ventriculoperitoneal
Assume patients who present to emergency with headaches associated with a ventricular shunt, has infection/blockage. Refer as an emergency. Associated drowsiness is a particular pointer to blockage.
Complications & Prognosis
Shunt Complication
- Infection
- Blockage
- Disconnection
- Pulmonary hypertension
References
Royal Children’s Hospital Melbourne



Members only discussions coming soon…