

Paediatric Viral Cutaneous Infection

Classical Exanthem
Overview
Exanthem refers to the cutaneous manifestation of a viral illness (enanthem is the manifestation in the mouth). Historically, 6 exanthems have been recognised, 4 of which are viral. However, obviously there are much more common exanthems.
The six described are:
- Measles (measles virus)
- Scarlet fever (streptococcus pyogenes) – this is a bacterial infection and will not be discussed here
- Rubella (togavirus virus)
- ?
- Erythema infectiosum (Parovirus B19)
- Roseola infantum (human herpes virus 6 and 7)
Human herpes virus 6 and 7 also cause Pityriasis Rosea.
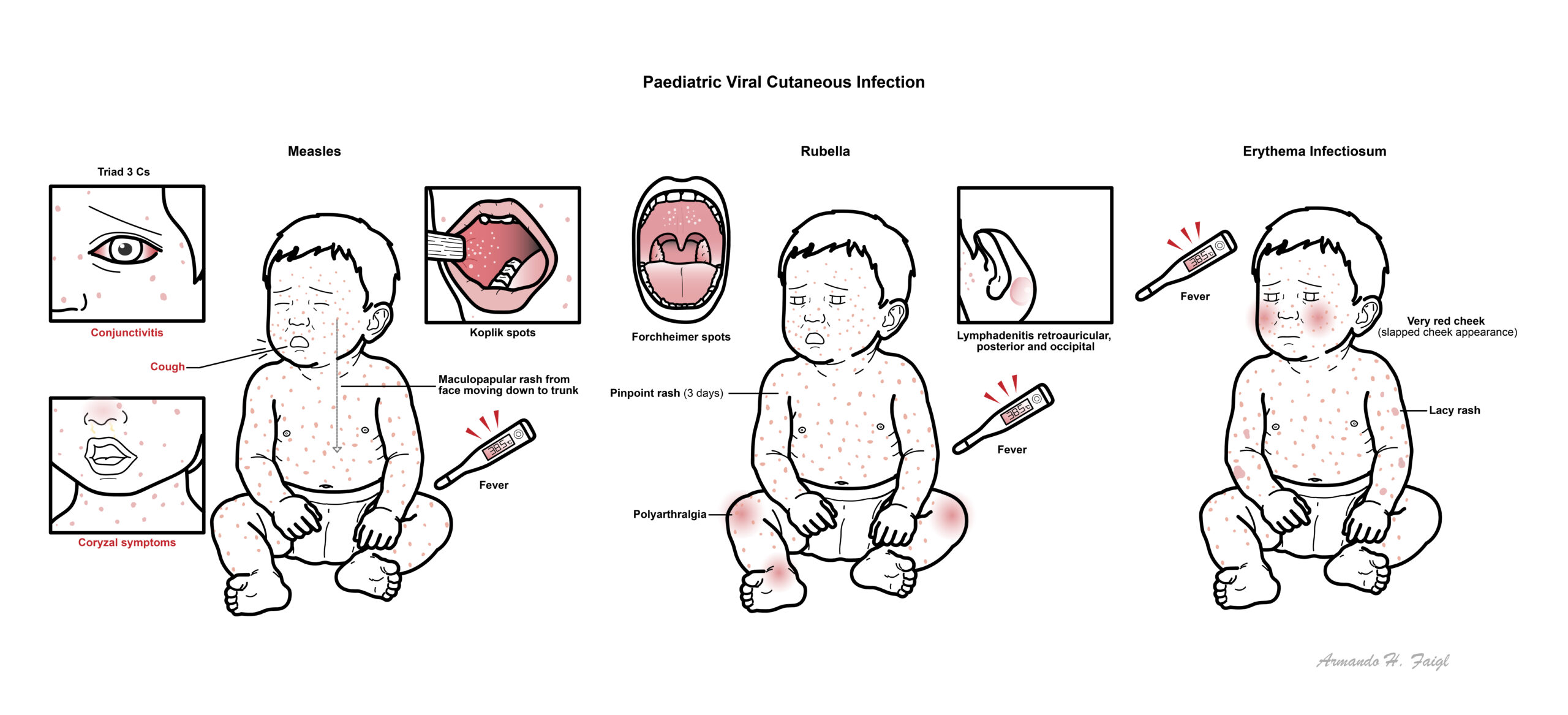
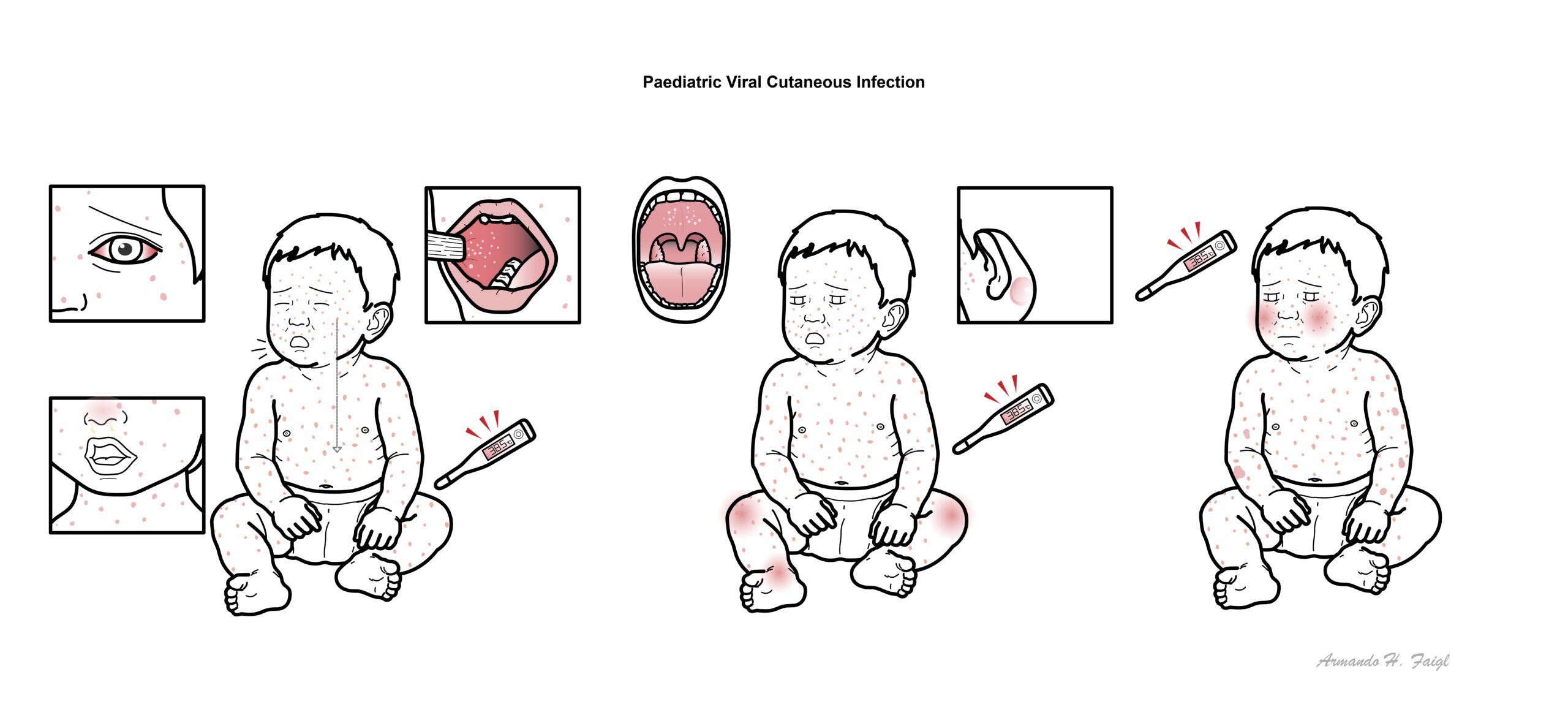
Measles
Overview
Also known as rubeola or first disease it is a highly contagious infection. Presents as an acute exanthematous febrile illness accompanied by conjunctivitis and koplik spots.
Aetiology
- Measles virus
- Prodromal phase
- Coryzal symptoms
- Marked malaise
- Conjunctivitis
- Fever
- Koplik spots
- Exanthema phase
- Maculopapular rash from face moving down to trunk
- Convalescent stage
- Rash fades
- Persistent cough improving
Triad 3 Cs for prodrome phase Cough, Coryza and Conjunctivitis then Koplik spots.


- Vaccination to prevent the disease is important
- Supportive treatment
- Isolation (its contagious)
- If Immunocompromised Antiviral and Vitamin A
- Encephalitis
- Subacute sclerosing panencephalitis
- Conjunctivitis
- Gastrointestinal – diarrhoea
- Otitis media
- Thrombocytopaenia → DIC
Complications common if malnourished or immunocompromised.
Rubella
Overview
Generally a mild illness, but can cause devastating congenital infection. Also known as german measles or third disease. It is a minor illness in children and adults, but devastating when transmitted in utero.
Congenital rubella is still the most important cause of blindness and deafness in the neonate.
Aetiology
- Togavirus
Clinical presentation
- Fever
- Lymphadenitis retroauricular, posterior and occipital
- Pinpoint rash from face moving down to trunk (~3 days hence also called the 3 day measles)
- Forschimer spots
- Polyarthralgia
Hallmark of Rubella Lymphadenitis retroauricular, posterior and occipital.

Management
- Supportive management
Congenital Rubella
Infection of the mother in the first trimester can lead to abortion or stillbirth, or to fetal malformation, including congenital heart disease, deafness and blindness (cataract or glaucoma).
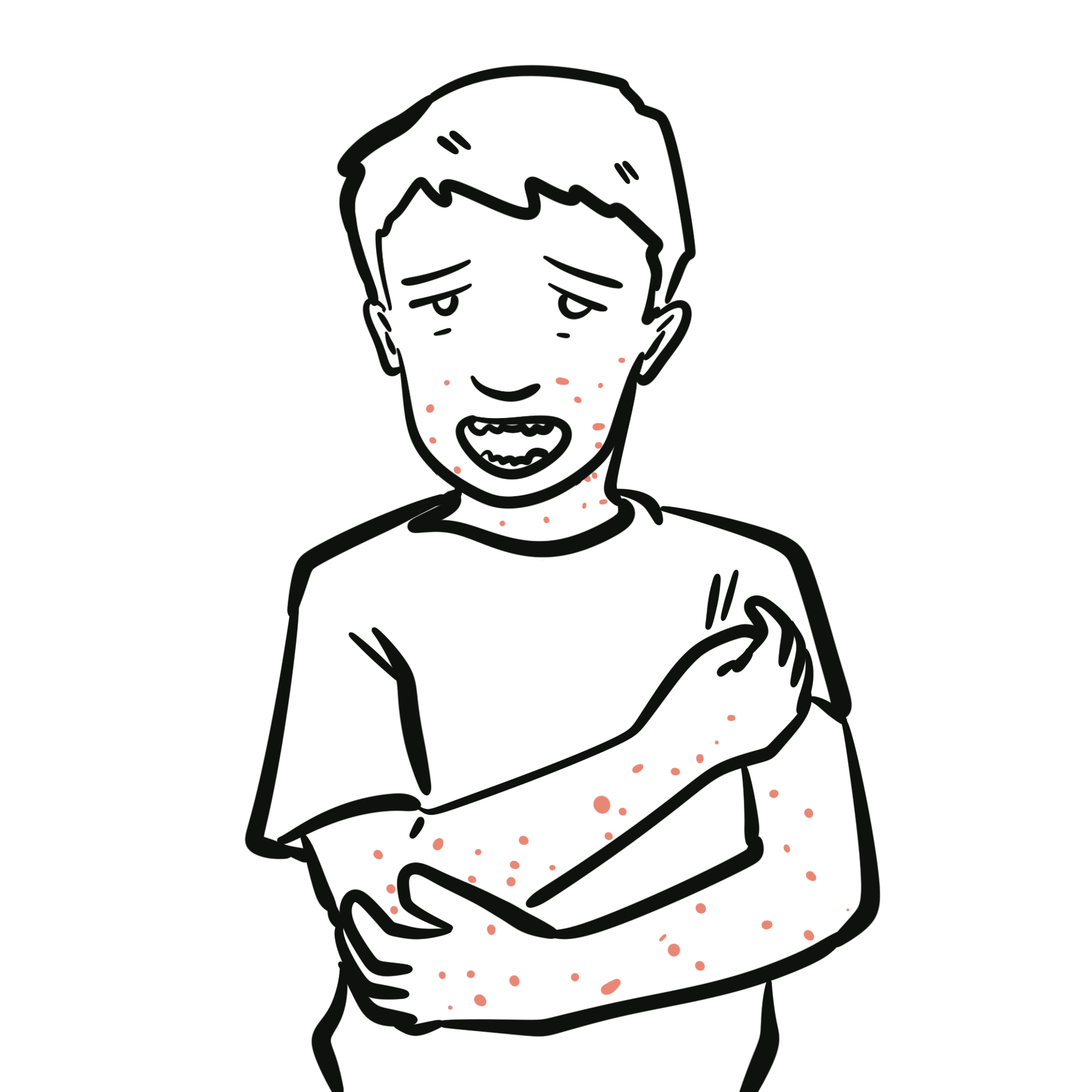
Erythema Infectiosum
Overview Also known ‘slapped cheeck’ or fifth disease.
Aetiology
- Parovirus B19
Clinical presentation
- School aged
- Very red cheek (slapped cheek appearance)
- Lacy eruption mainly on the extremities
- Arthritis

Management
- Supportive management
Complications
- Aplastic anaemia
- Thrombocytopenia and neutropenia neutropenia.
- Parvovirus B19 infection in pregnancy can cause fetal hydrops
Papular Purpuric Gloves and Socks Syndrome is also caused by parvovirus B19 and presents with erythema, oedema, petechaie and purpura of palms and soles + burning and pruritus. It is self limiting and occurs in children and adolescents.
Roseola Infantum
Overview
Also known as exanthema Subitum and sixth disease.
Aetiology – Human herpes 6 virus
Clinical presentation
- 6months – 3 years
- Fever ~41C for three days followed by
- Generalised maculopapular rash
- Circular to elliptical rose red maculopapular rash involving the trunk
| Remember |
High grade fever for 3 days (maybe URTI) which progresses to maculopapular rash all over body.

Complications
- Seizures
Pityriasis Rosea
Overview
Pityriasis Rosea is a self-limiting skin rash thought to be caused by herpesvirus 6 or 7. Herald patch is often the primary lesion followed by additional similar smaller lesions around. Herald patch often misdiagnosed initially as a tinea infection.
Aetiology
- Human herpesvirus 6 or 7
Clinical Presentation
- Herald patch on the trunk may present first
- Smaller similar lesions after

Investigation
- Differentiate from tinea (fungal) using KOH
Management
- Resolves spontaneously
- Watchful waiting
Molluscum Contagiosum
Overview
Molluscum contagiosum is a common viral skin infection of childhood that causes localised clusters of epidermal pearly papules with central umbilication
Aetiology
- Poxvirus
Clinical presentation
- Small, pearly papules with central umbilication
- Skin lesions occur on any part of the skin surface
- Conjunctivitis if around eyelids

Management
- Supportive treatment – each lesion lasts ~7days
- Deroofing of the lesion with a 21-gauge cutting-edged needle and wiping out the contents.
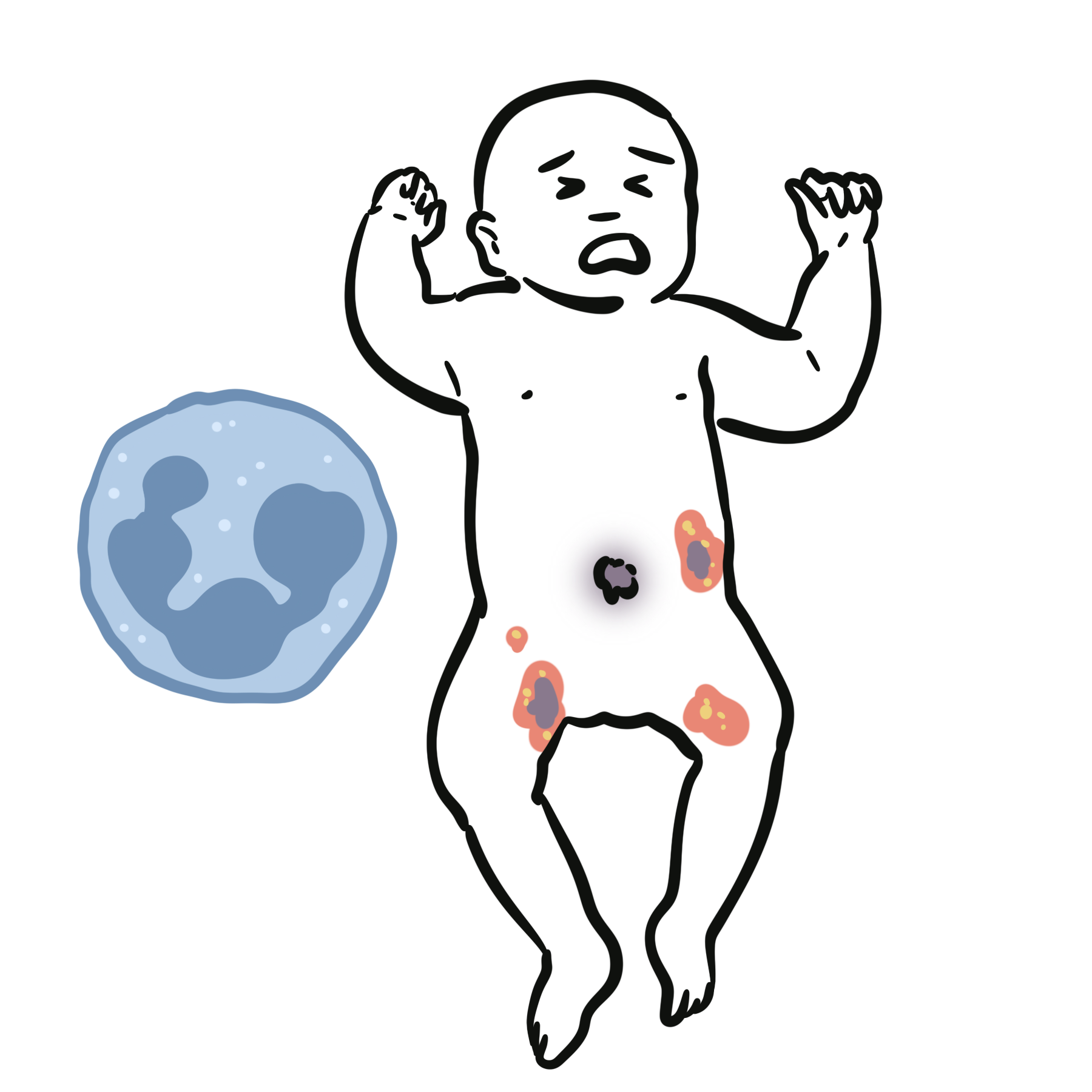
Hand-Foot and Mouth Disease
2 year old infant bought in with vesicular rash on her hand, foot and mouth.
Overview Mild vesicular eruption caused by a Coxsackie A virus.
Aetiology
- Coxsackievirus A16
A child presenting with fever and vesicles likely has chickenpox, hand foot and mouth or herpes simplex.
Clinical presentation
- <10 years old +/- adults
- 1-2 weeks after and URTI
- Ellpitical grayish vesicles, pustules and erosions on hand feet and buttocks



Management
- Supportive care
Complications
- Myocarditis
- Pneumonia
- Encephalitis
Adenovirus
A 12 year old boy present with fever sore throat and follicular conjunctivitis
Clinical Presentation
- Fever
- Pharyngitis
- Follicular Conjunctivitis
| Acute follicular conjunctivitis (usually viral) |
| Adenovirus |
| Herpes zoster virus |
| Epstein-Barr virus |
- Streptococcus pharyngitis
- Viral PCR
Management
- Supportive treatment
Warts
Overview
Benign epidermal tumors caused by multiple types of human papillomaviruses. The common wart (verruca vulgaris) occurs particularly on hands, knees and elbow.
Aetiology
- Human Papilloma Virus
Clinical Presentation
- Plane or flat warts, 1–3-mm, pink or brown, barely raised papules, occur on the face
- Plantar warts occur particularly over pressure points on the soles and can be differentiated from calluses by a loss of skin markings over the skin surface.
- Anogenital warts may be acquired from maternal infection during delivery but their presence in older children raises the suspicion of sexual abuse
Management depends on type and number of warts, the location on the body, and the age of the patient
- No cure
- Supportive treatment – most resolve themselves
- Salicylic acid with regular paring and occlusion.
- Cryotherapy (topical liquid nitrogen) + salicylic acid
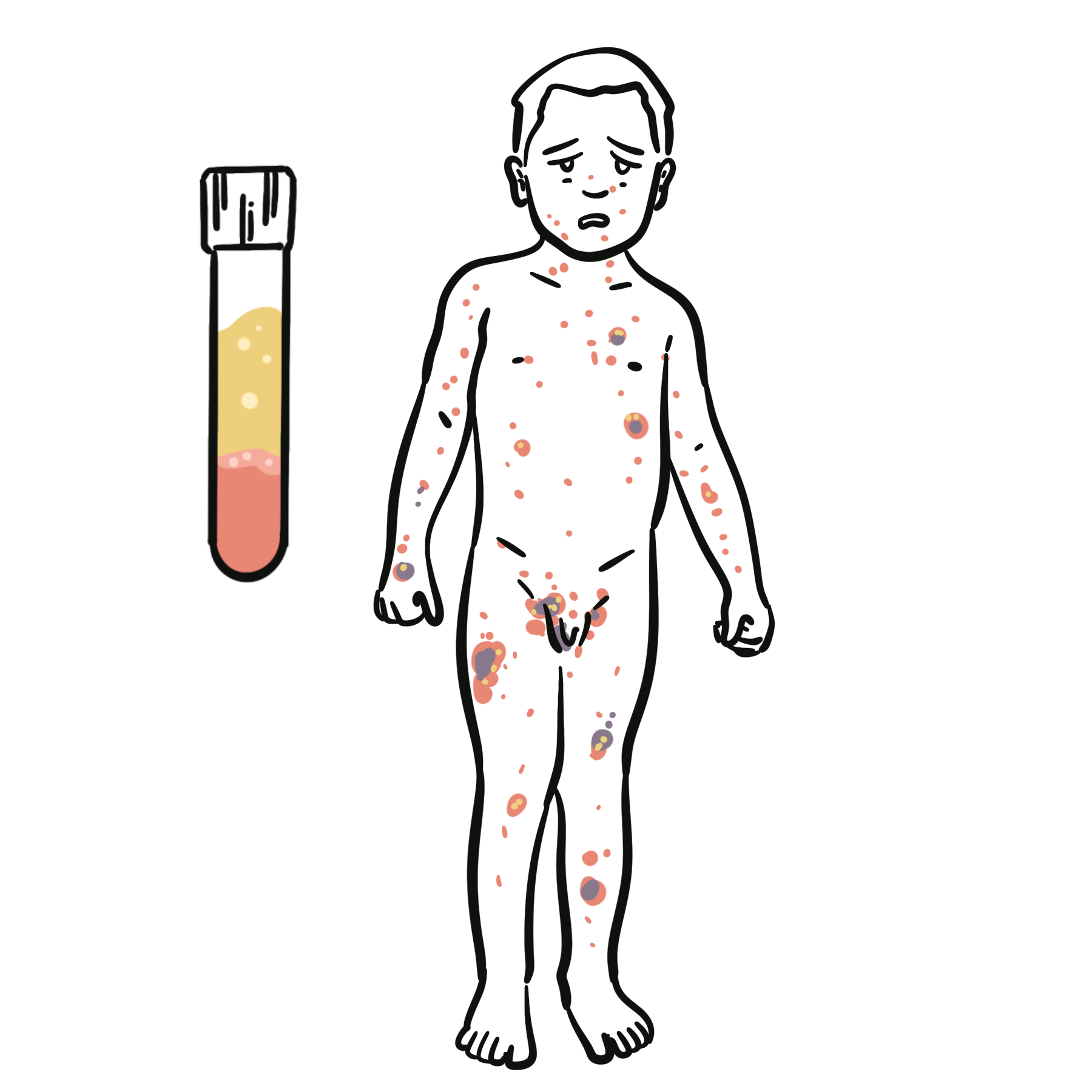
Chickenpox
Overview
Common, contagious viral infection involving the skin characterised by pruritic vesicles which eventually crust over. Clinical reactivation later in life results in herpes zoster (shingles). It is transmitted by airborne spread.
A child presenting with fever and vesicles likely has chickenpox, hand foot and mouth or herpes simplex.
Aetiology
- Varicella Zoster Virus
Virus can become latent in sensory ganglia and reappears as herpes zoster (shingles) later in life.
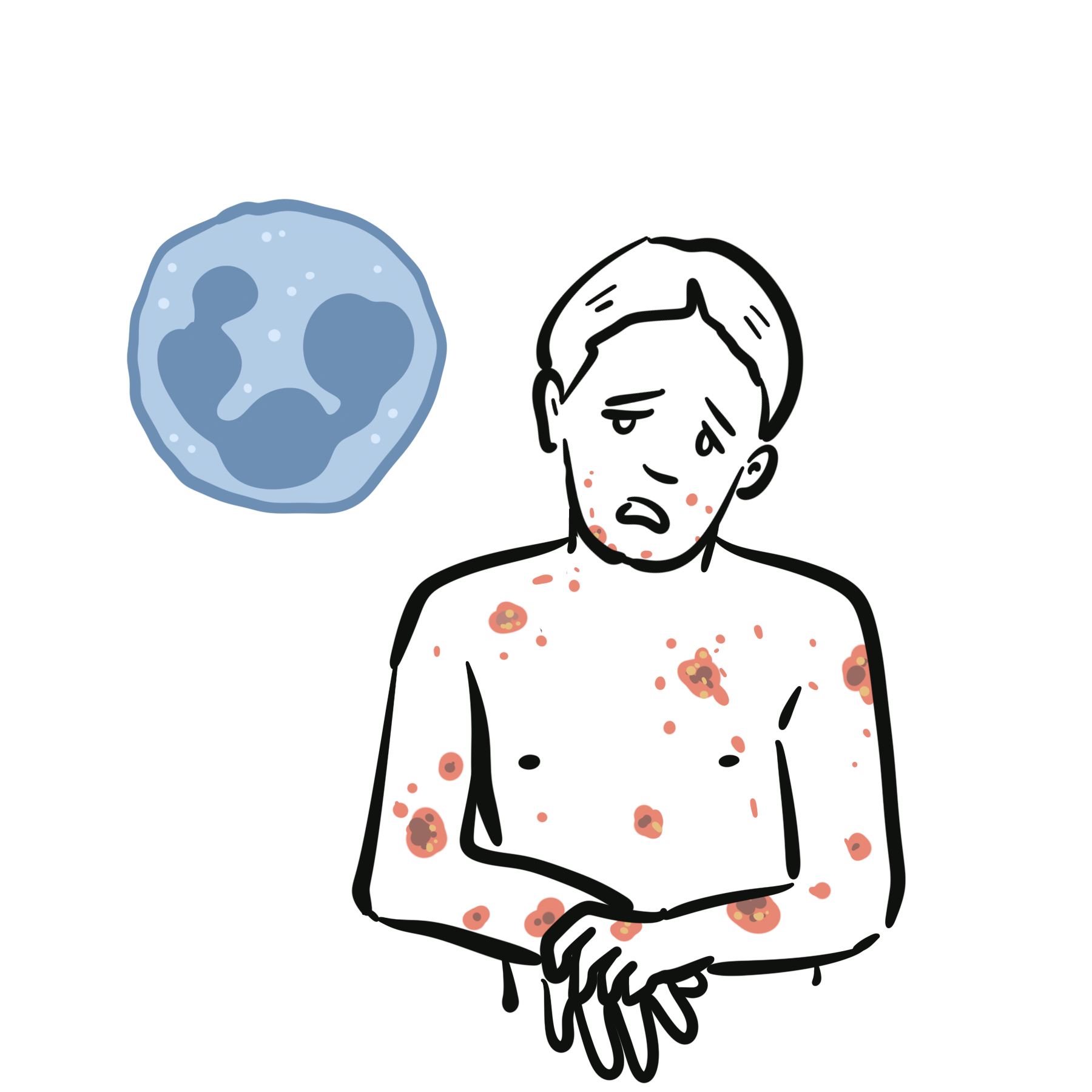
Clinical Presentation – all stages of rash is seen
- Prodromal symptoms 1-3 days – fatigue, headache, fever (this is more common in adults)
- Pruritic, erythematous maculopapular rash
- Rash begins in face and spreads to trunk and extremities
- Rash evolves into vesicles with narrow red halo “Dew drops on rose petals”
- Vesicles then crust
Adults can also present with chicken pox and these are often more severe.

Management
- Supportive
- Person is infective 2 days before rash appears and when rash crusts over
- Stay home, no school
- Paracetamol (avoid aspirin)
- Avoid scratching
- cut fingernails
- antihistamines
- Antivirals – aciclovir (usually for older children/adults who have severe chicken pox)
Complication
- Secondary bacterial skin infection from scratching
- Can leave pitted scars
Herpes simplex
A child presenting with fever and vesicles likely has chickenpox, hand foot and mouth or herpes simplex.
Overview
Primary Herpes simplex virus (HSV) infection in children is usually asymptomatic or non- specific. Herpetic gingivostomatitis is the most common specific clinical manifestation, occurring in 25% to 30% of cases.

Clinical presentation
- 1-3 years old
- Fever
- Ulcer on gums, tongue and palate
- Dehydration
- Anorexia
Management
- Fluids
- Oral lignocaine gel
- Acyclovir (for those who are immunocompromised)
Complications
- Encephalitis
- Eczema herpeticum
- System HSV infection in neonates
Infectious mononucleosis
Overview
Infectious mononucleosis is a febrile illness caused by the herpes (Epstein– Barr) virus. It can mimic diseases such as HIV primary infection, streptococcal tonsillitis, viral hepatitis and acute lymphatic leukaemia
Aetiology
- Ebstein Barr Virus
Classification
- Febrile
- Anginose
- Glandular
Clinical Presentation
- School age child, adolescents
- Fever
- Pharyngitis
- Fatigue
- Mylagia
- Headache
- Hepatosplenomegaly
- Lymphadenopathy
- Rash is polymorphous – non specific, occurs in about 5% of cases only.
- Rashes development are almost always related to antibiotics given for tonsillitis
- The secondary rash is most often precipitated by one of the penicillins, especially ampicillin or amoxycillin.
Infectious mononucleosis triad Sore throat, fever and lymphadenopathy.
Differential Diagnosis
- HIV infection
- CMV
- Toxoplasmosis
- Acute streptococcus pharyngitis
- Adenovirus
- Hepatitis
- Lymphoma
- Leukaemia
Investigations
- FBC – Lymphocytosis
- Blood film- atypical lymphocytes.
- Positive Monospot test for heterophil antibody
- Serum EBV-specific antibodies
Management
- NSAIDS
- Aspirin
- Fluids
- Nutrition
- +/- acyclovir
- If airway compromise – ENT review + steroids to decrease oedema
Morbilliform eruption may occur after treatment with ampicillin.
Complications
- Splenic rupture
- Airway obstruction
- Hepatitis
- Rash (ampicillin related)
- Burkitt’s lymphoma
- Oral hairy leukoplakia
Advise against alcohol, fatty foods, continued activity, especially contact sports (risk of splenic rupture).




Members only discussions coming soon…