

Melanoma
Overview
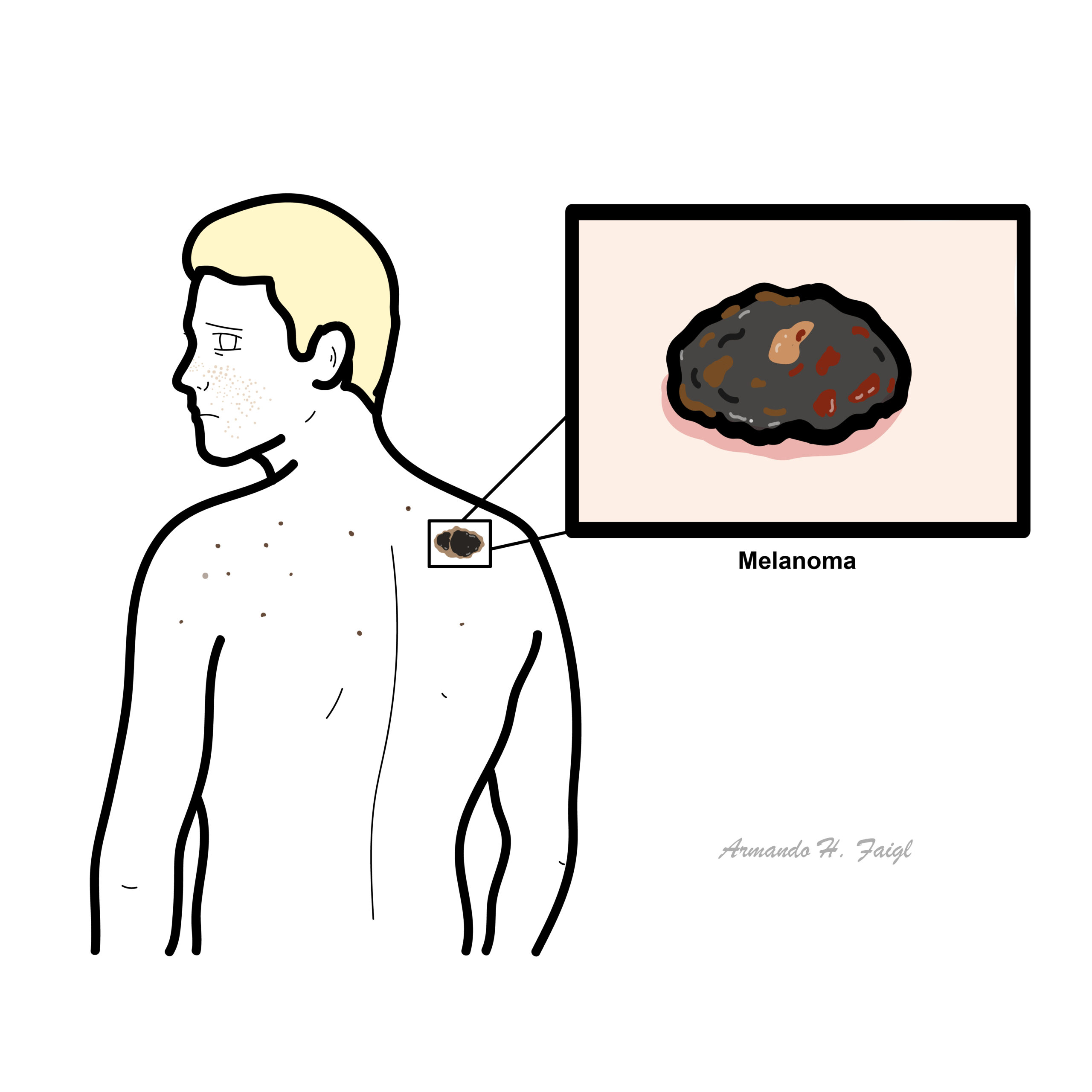
Melanoma accounts for 4 percent of all dermatological cancer. Melanoma has the highest mortality rate of all dermatological cancers, only 14 percent of patients with metastatic melanoma survive for five years. Melanoma is one of the most common cancers in young adults.
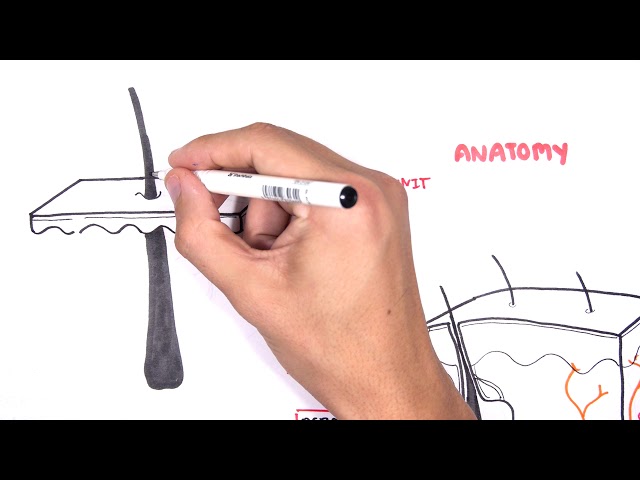
Anatomy & Physiology
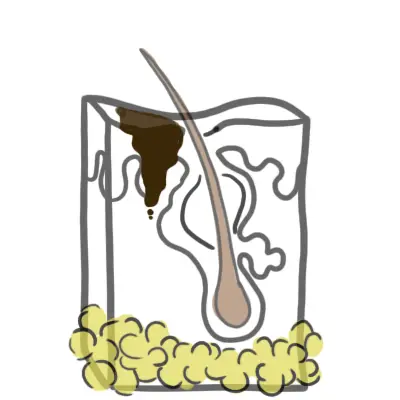
The skin consist of three layers, from superficial to deep:
- Epidermis
- Dermis
- Papillary layer
- Reticular layer
- Hypodermis (some don’t classify it as skin)
The epidermal layer are made up mainly of keratinocytes, which are squamous epithelial cells high in keratin (protein). Other cells residing in the epidermis include:
- Melanocytes – produce melanin
- Langerhan cells – immune cell, basically a dendritic cell of the skin
- Merkel Cells – tactile cells for sensation
Melanocytes are mature melanin-forming cells found in many parts of the body (eye, ear, hair, heart, bone), but especially in the skin. Through a process called melanogenesis, these cells produce melanin, which is a pigment found in the skin, eye and hair. Vitamin D and UV light stimulate melanocytes to produce melanin.
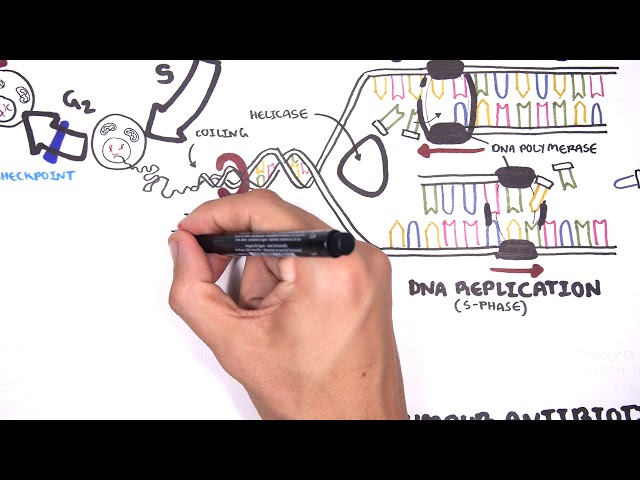
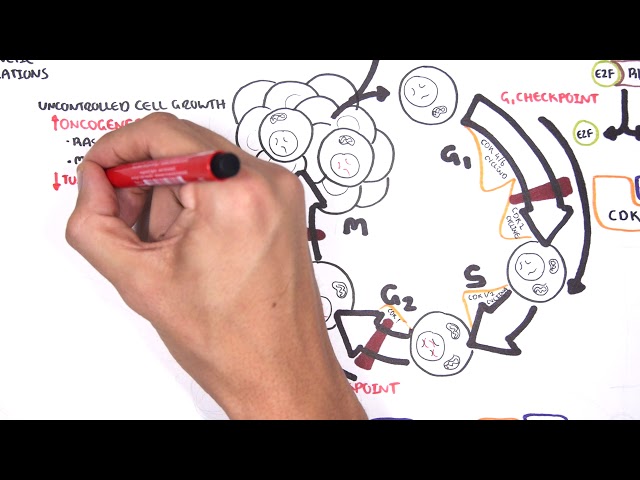
Pathophysiology
- Melanoma arises from melanocytes
- Genetics and environmental factors play a role in the pathogenesis
- A proportion of melanoma arise from pre existing naevi
Mutated BRAF and NRAS genes are most common in superficial spreading and nodular melanoma.
Classification
Different types of Melanoma
- Superficial spreading (most common)
- Nodular (most dangerous)
- Lentigo maligna
- Acral lentiginous
| Pathological Differences between Benign and Malignant tumours | |
| Malignant | Benign |
| Invasive | Non-Invasive |
| Poorly differentiated | Well Differentiated |
| High mitotic rate | Normal mitotic rate |
| Non-capsulated | Capsulated |
| Usually large growth | Usually small growth |
| Not well circumscribed | Well circumscribed |
Clinical Manifestation
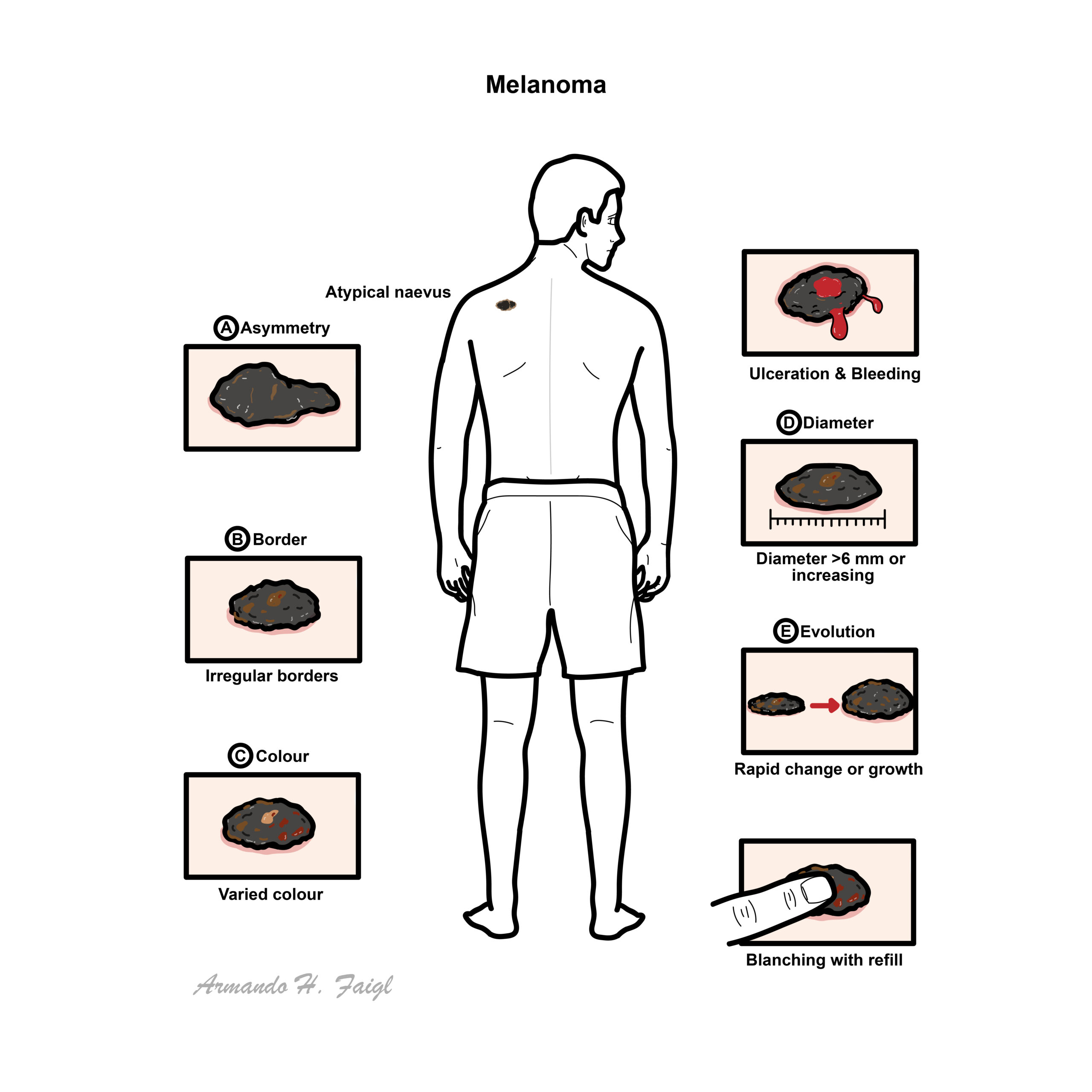
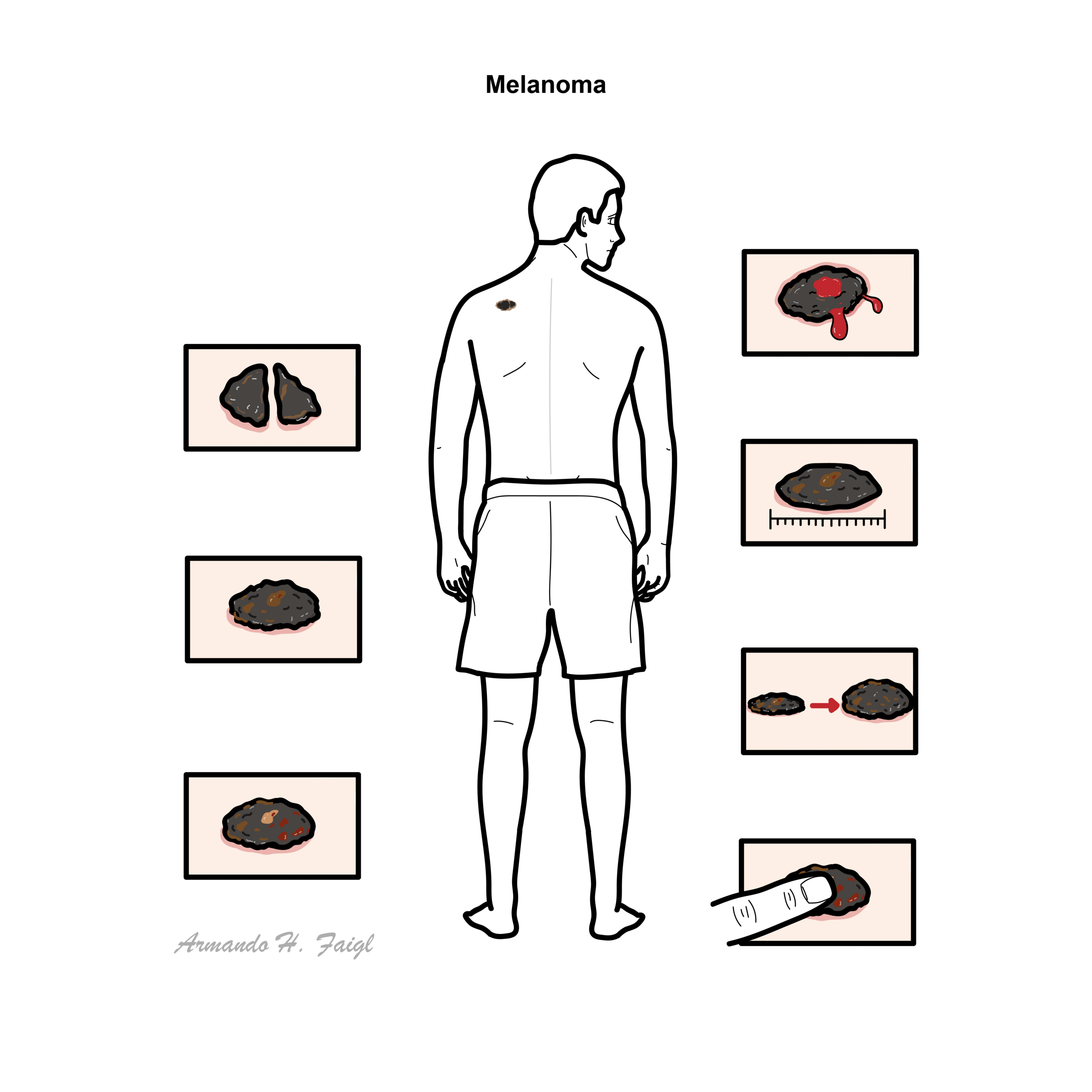
- Atypical naevi
- Ulceration and bleeding
- Constitutional symptoms
Examination – ABCDE
- A – asymmetry
- B – borders (irregular and/or distinct)
- C – colour (varied)
- D – Diameter (increasing or >6mm)
- E – Elevation and Evolution (most important as in changing rapidly/growing)
Blanching. Press down on the lesion for ~3 seconds. Release if pale and refills there is a vascularity involved.
Diagnosis
- Excision biopsy is preferred
- Remove the entire lesion with a narrow clinical margin, usually approximately 2 mm.
- Partial punch or incisional biopsy may be used when complete excision is impractical, such as a large facial, acral or mucosal lesion.
- Histopathology confirms melanoma and should report:
- Melanoma subtype
- Breslow thickness
- Ulceration
- Mitotic activity
- Microsatellites
- Peripheral and deep margins.
Staging investigations
- Stage using the AJCC TNM system:
- T: thickness and ulceration of the primary tumour
- N: regional lymph-node involvement
- M: distant metastases
- Sentinel lymph-node biopsy should be discussed for melanoma ≥0.8 mm thick, particularly where ulceration or other high-risk features are present.
- Enlarged or abnormal lymph nodes: ultrasound followed by fine-needle aspiration or core biopsy.
- Routine imaging is generally unnecessary for thin, asymptomatic, node-negative melanoma.
- CT, PET-CT and brain MRI may be used for high-risk, stage III or suspected metastatic disease.
- Test for BRAF V600 mutation in resected high-risk or advanced melanoma when targeted treatment may be considered.
- Seborrhoeic keratosis
- Pigmented basal cell carcinoma
- Actinic keratosis
- Benign melanocytic naevi
- Spitz naevus
- Haemangioma
Squamous cell carcinoma is not a good differential because it is not pigmented.
- Dermatoscope
- Skin Biopsy
- Chest X-ray for metastasis
1.4cm depth is dangerous.
Staging
| Clark’s Staging – Important histologically | |
| Clark’s Level | Histological characteristic |
| I | Confined to the epidermis “in situ” |
| II | Invasion of the papillary dermis |
| III | Filling of the papillary dermis |
| IV | Invasion of the reticular dermis |
| V | Invasion of the deep, subcutaneous tissue |
| Breslow’s Staging – Important Prognostically | |
| Breslow’s Thickness | Depth of tumour invasion |
| I | ≤0.75mm |
| II | 0.75-1.5mm |
| III | 1.51-2.25mm |
| IV | 2.26-3.0mm |
| V | >3.0mm |
Treatment
Localised melanoma
- Wide local excision is the main treatment.
- Consider sentinel lymph-node biopsy at the time of definitive excision when indicated.
- Surgery is usually curative for thin, localised melanoma.
Stage II melanoma +/- III
- Wide local excision ± sentinel lymph-node biopsy.
- For resected stage IIB or IIC melanoma, consider adjuvant anti-PD-1 immunotherapy, such as:
- Pembrolizumab
- Nivolumab
- Observation with structured follow-up remains appropriate for some patients after discussion of recurrence risk and treatment toxicity.
Unresectable stage III or stage IV melanoma
- Immune-checkpoint inhibitors:
- Pembrolizumab
- Nivolumab
- Nivolumab plus ipilimumab
- Nivolumab plus relatlimab
- BRAF/MEK inhibition for BRAF V600-mutated disease:
- Dabrafenib plus trametinib
- Encorafenib plus binimetinib
- Vemurafenib plus cobimetinib
- Selected local treatments:
- Surgical resection of limited metastases
- Stereotactic radiotherapy or surgery for brain metastases
- Radiotherapy for painful bone disease or local symptom control
- Intralesional treatment for selected accessible lesions
- Chemotherapy has limited activity and is generally reserved for later-line or palliative treatment.
- Early supportive and palliative care should accompany treatment of advanced disease.
Complications & Prognosis
- Local recurrence at or near the original lesion
- Satellite or in-transit metastases
- Metastases
- Neurological deficits, seizures or raised intracranial pressure from brain metastases
- Pathological fractures or spinal cord compression
- Pain, bleeding, ulceration, cachexia and functional decline.
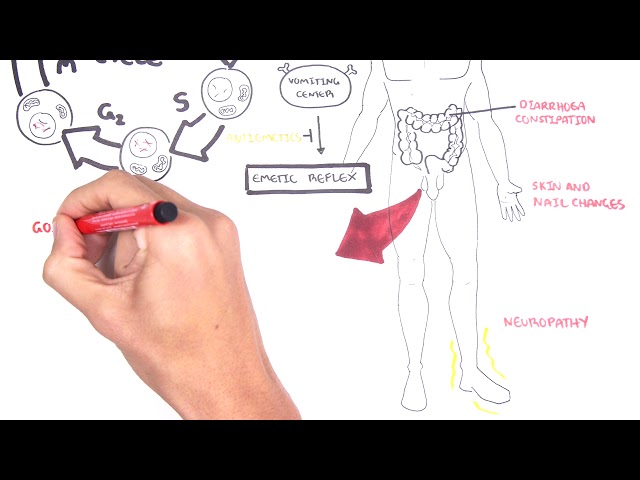
Treatment-related
- Surgical wound infection, scarring or graft complications
- Lymphoedema following lymph-node surgery
- Immune-checkpoint toxicity:
- Dermatitis
- Colitis
- Hepatitis
- Pneumonitis
- Thyroiditis, hypophysitis or adrenal insufficiency
- BRAF/MEK inhibitor toxicity:
- Fever
- Rash
- Arthralgia
- Cardiac dysfunction
- Ocular toxicity.
- Thin, non-ulcerated, node-negative melanoma generally has an excellent prognosis.
- Thick or ulcerated melanoma, positive lymph nodes, in-transit disease and distant metastases carry progressively higher recurrence and mortality risks.
- Modern immunotherapy and BRAF/MEK-targeted treatment have substantially improved outcomes in advanced melanoma, although resistance and relapse can occur.
- In Australia, the overall five-year relative survival for melanoma was 94% for people diagnosed during 2017–2021; this overall figure includes the large proportion diagnosed at an early stage and does not represent the prognosis of metastatic melanoma.
References
- Amaral T, Ottaviano M, Arance A, Blank C, Chiarion-Sileni V, Donia M, et al. Cutaneous melanoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025;36(1):10–30. doi:10.1016/j.annonc.2024.11.006.
- Cancer Council Australia Melanoma Guidelines Working Party. Clinical practice guidelines for the diagnosis and management of melanoma [Internet]. Sydney: Melanoma Institute Australia and Cancer Council Australia; 2026.
- PDQ Adult Treatment Editorial Board. Melanoma treatment (PDQ): health professional version [Internet]. Bethesda: National Cancer Institute; updated 2025 May 2.
- Sladden MJ, Balch C, Barzilai DA, Berg D, Freiman A, Handiside T, et al. Updated evidence-based clinical practice guidelines for the diagnosis and management of melanoma: definitive excision margins for primary cutaneous melanoma. Med J Aust. 2018;208(3):137–142. doi:10.5694/mja17.00278.
- Cancer Australia. Melanoma of the skin statistics [Internet]. Canberra: Australian Government; updated 2025 Dec 18.






Members only discussions coming soon…