

Atopic Dermatitis (Eczema)

Overview
Atopic dermatitis is a chronic highly pruritic (itchy) inflammatory skin disease.Atopic dermatitis and eczema are often used synonymously. Atopic dermatitis primarily affect young children and is often associated with other atopic disorders, such as allergic rhinitis and asthma. The prevalence of atopic dermatitis has doubled or tripled in industrialised countries during the past three decades. Not only are patients affected by the social stigma of a visible skin condition, but the intense itching characteristic of the disease often leads to significant sleep as well.
Atopic dermatitis affects approximately 5 to 20 percent of children worldwide. The incidence of atopic dermatitis appears to be increasing. It may occur in any race or geographic location, although there appears to be a higher incidence in urban areas and developed countries, especially Western societies.
Anatomy
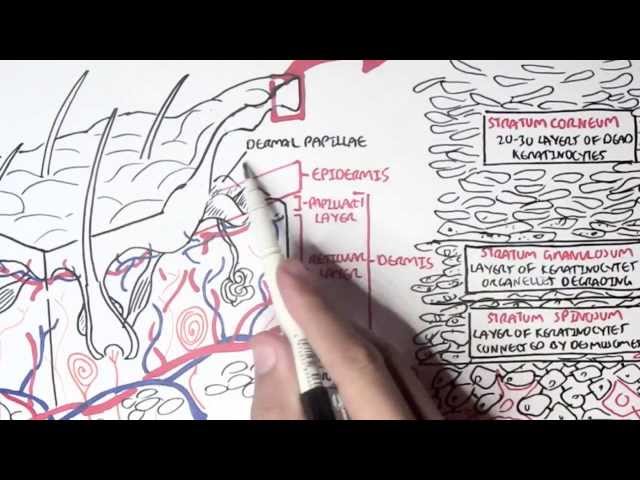
The skin consist of three layers, from superficial to deep:
- Epidermis
- Dermis
- Papillary layer
- Reticular layer
- Hypodermis (some don’t classify it as skin)
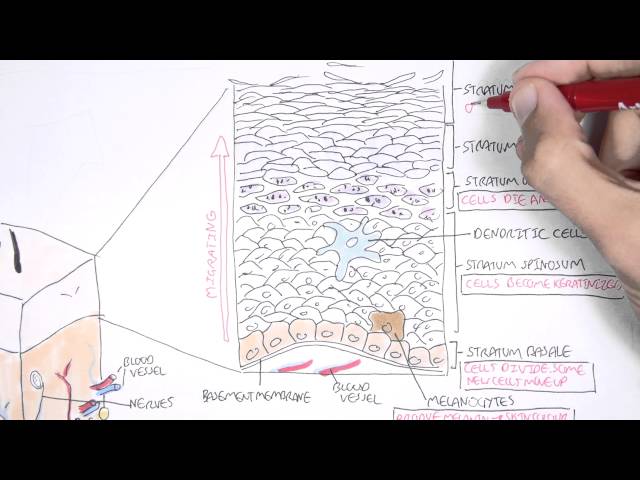
The epidermal layer are made up mainly of keratinocytes, which are squamous epithelial cells high in keratin (protein). Other cells residing in the epidermis include:
- Melanocytes – produce melanin
- Langerhan cells – immune cell, basically a dendritic cell of the skin
- Merkel Cells – tactile cells for sensation
The epidermis itself can be further divided into 4 or 5 layers, from top to bottom:
- Stratum corneum
- +/- Stratum lucidum
- Stratum granulosum
- Startum spinosum
- Stratum basale
These layers are bound firmly thanks to the Filagrin gene which is responsible for making proteins important for proper skin barrier function, particularly structural proteins in the stratum corneum and granulosum, that help bind keratinocytes together.
Aetiology & Risk Factors
Aetiology
Atopic dermatitis can be though of a complex genetic disease arising from several gene gene and gene-environment interactions.
Genes
Many genes have been associated with atopic dermatitis, especially what’s known as the filagrin gene on chromosome 1. 50% of people with atopic dermatitis carry a mutated filigrrin gene . The filagren gene encodes a structural protein essential for skin barrier formation.
Environment
There is thought because of a more westernised industrialised lifestyle more people are developing eczema. This compliments the so called hygiene hypothesis which states that the decrease in early childhood exposure to infections, has increased susceptibility to atopy, tendency towards allergy.
| Risk Factors |
| Age <5 years |
| Family History |
| Allergic rhinitis |
| Asthma |
| Antihelminth treatment |
Pathophysiology
Two main hypothesis proposed in atopic dermatitis.
Immunological hypothesis (inside out hypothesis)
1. T helper cells differentiate into T helper 1 (Th1) or T helper 2 (Th2)
- Th1 promotes cell mediated immunity (Inflammation)
- Th2 promotes humoral immuniy (antibodies)
2. Imbalance of T cells. Th2 differentiation predominate
3. Th2 produces:
- IL 4 -> positive loop to produce more Th2
- IL 5 -> stimulates B-cell antibody production
- IL 13 -> stimulates B cell class switching to IgE (Elevated IgE are present in only 50% of patients with AD).
4. Increase in IgE leads to hypersensitivity -> allergic response
5. Cytokine production also down regulates the production of skin antimicrobials cathelicidins and defences -> predisposes patients to infections (S. aureus)
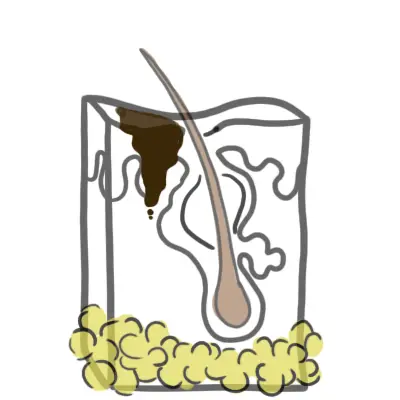
The skin barrier Hypothesis (outside in hypothesis)
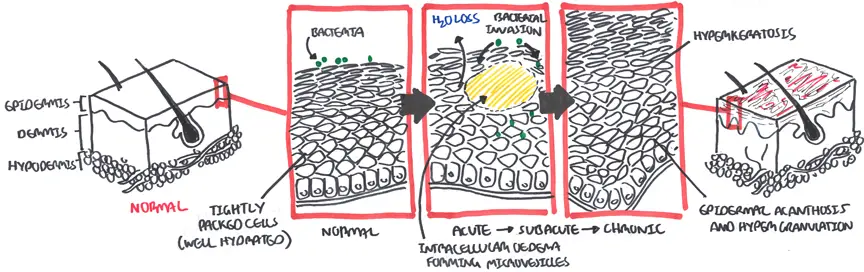
1. The epidermis is the first line of defence between the body and the environment. The skin barrier keeps environmental irritants, allergens, and microbes from entering the body and prevents excessive water loss.
2. Filagrin gene is responsible for making proteins important for proper skin barrier function, particularly structural proteins in the stratum corneum and granulosum that help bind keratinocytes together.
3. Mutation in the filagrin gene results in skin barrier dysfunction and water loss which causes eczema.
4. Impaired skin barrier also increases penetration of allergens into skin allergic sensitisation to asthma and hay fever.
Histology/Pathology
Pathology
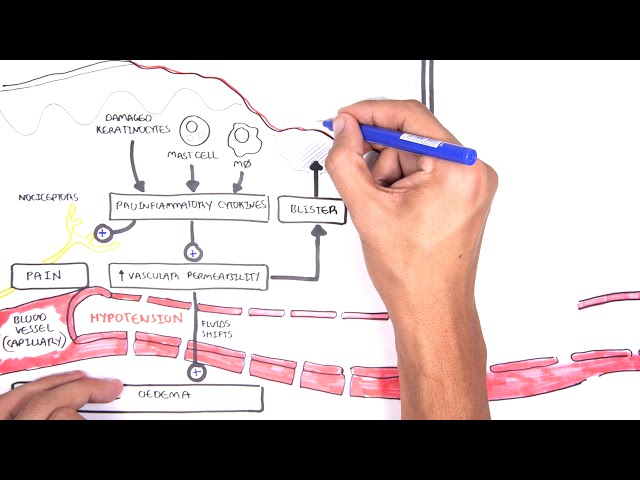
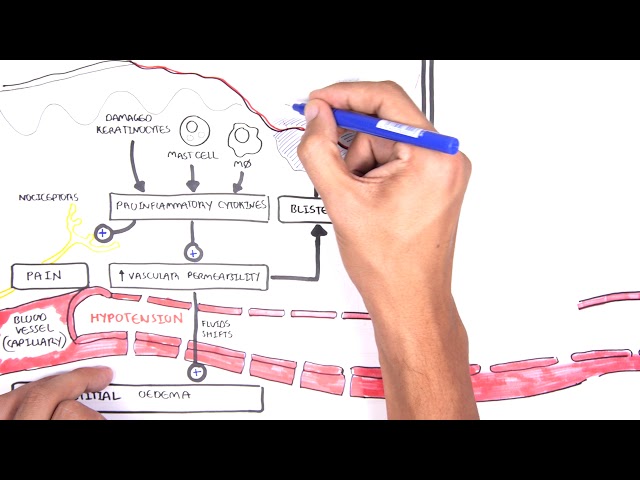
Epidermal intercellular oedema (spongiosis) and a prominent perivascular infiltrate of lymphocytes, monocyte, macrophages, dendritic cells and a few eosinophils in the dermis. In subacute, chronic stages—epidermis is thickened and its upper layer is hypertrophied.
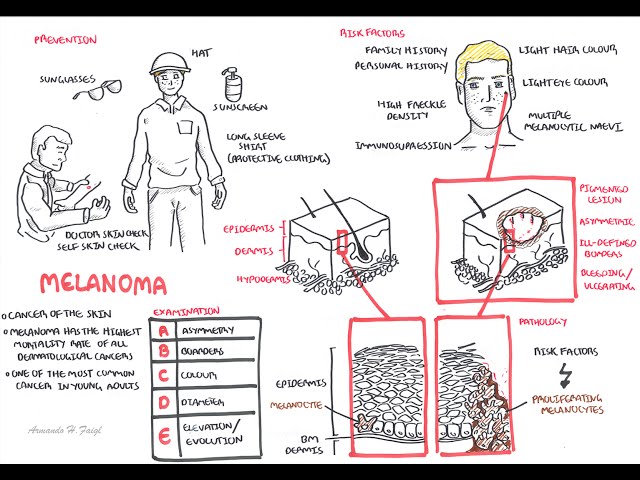
Clinical Manifestations
- Pruritis (itching)
- Xerosis (dry skin)
- Excoriations (scratch marks)
- Hypopigmentation of affected areas
During Flare ups
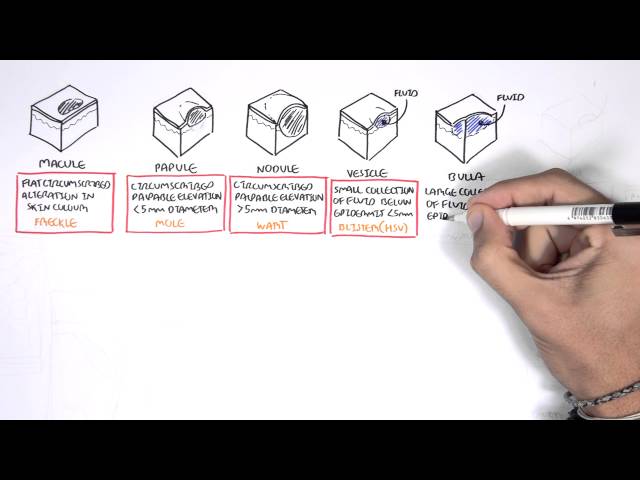
- Erythema
- Scaling
- Vesicles
- Papules
Chronic
- Lichenification
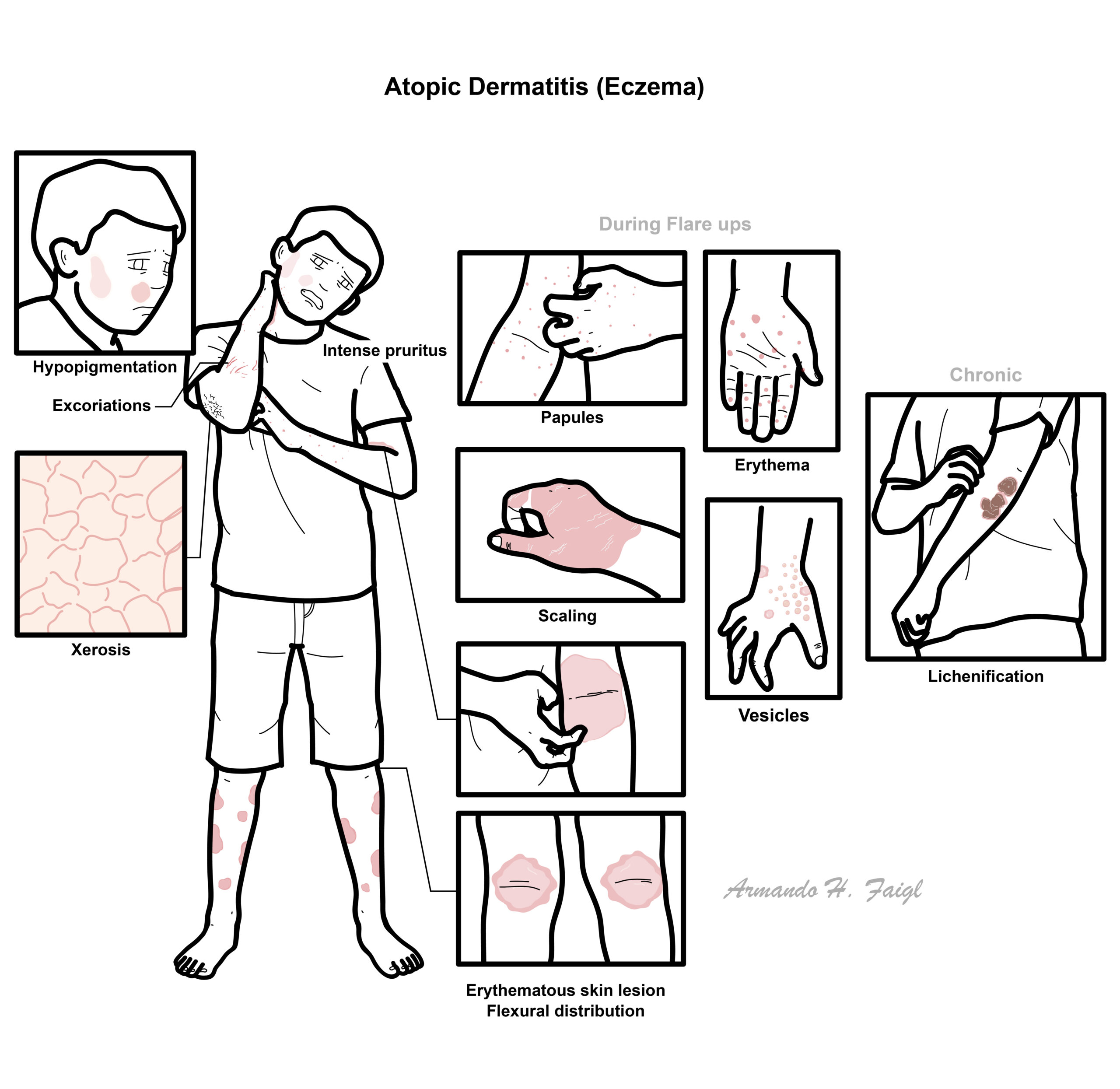
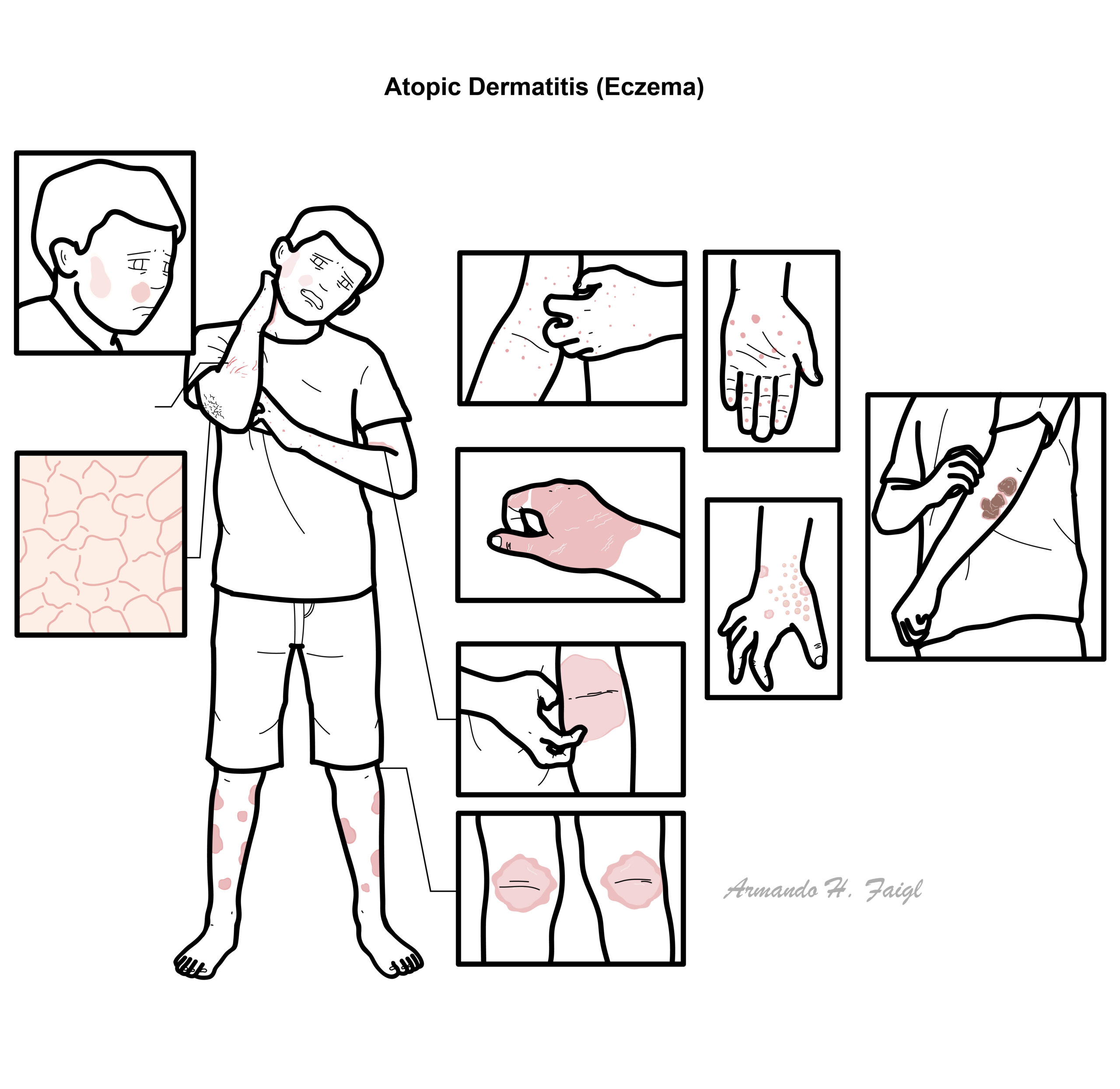
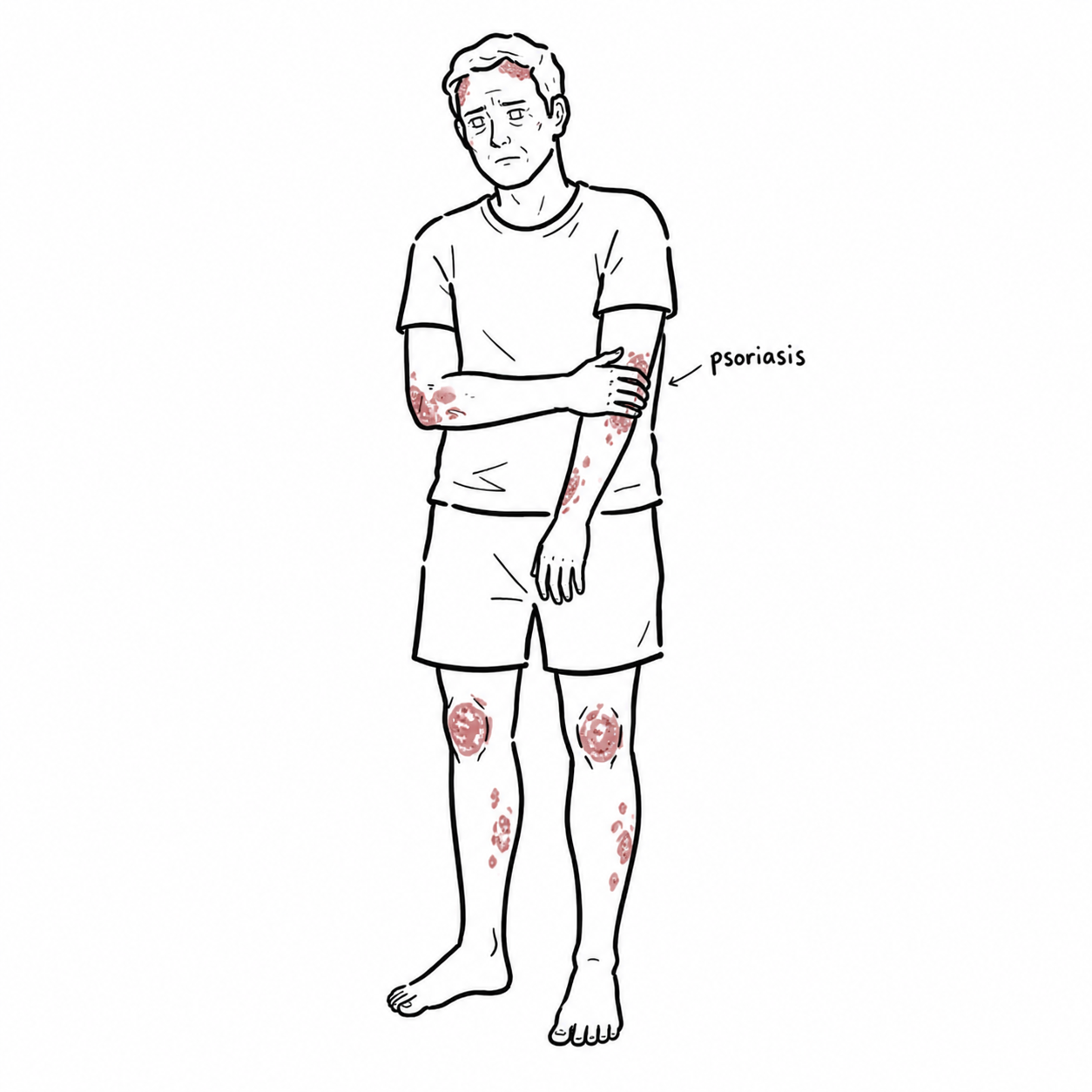
Atopic Dermatitis affect mainly flexor surfaces, this differs to psoriasis which classically affect extensor surfaces.
Diagnosis
- Clinical Diagnosis of Atopic Dermatitis
- Allergy testing (to detect potential triggers and exacerbating facotrs of the dermatitis)
- Serum IgE
- Skin Biopsy (differentiate between contact and allergic dermatitis)
The diagnosis of atopic dermatitis is clinical, based upon history, morphology and distribution of skin lesions, and associated clinical signs. There is no specific diagnosis and it is controversial but mainly includes:
1. Evidence of pruritic skin
2. In addition to itchy skin, three or more of the following:
- History of skin creases being involved.
- History of asthma or hay fever
- The presence of generally dry skin within the past year.
- Symptoms beginning <2 years of age.
- Visible dermatitis involving flexural surfaces. For children under four years of age, this criterion is met by dermatitis affecting the cheeks or forehead and outer aspects of the extremities.
Pruritic (Itchy) skin lesion
- Contact dermatitis
- Scabies
Non pruritic skin lesion
- Seborrhoeic dermatitis
- Psoriasis
Seborrhoeic dermatitis is a common, chronic or relapsing form of eczema/dermatitisthat mainly affects the scalp and face. It can be associated with psoriasis. Dandruff is an uninflamed form of seborrhoeic dermatitis.
Treatment
Education/trigger avoidance: avoid soaps, fragrances, overheating, wool and known irritants; use lukewarm rather than hot water.
Emollients: thick fragrance-free moisturiser/ointment several times daily and immediately after bathing; continue even when eczema is controlled. Topical corticosteroids for flares:
- Apply once or twice daily to active eczema until clear.
- Mild potency: face, neck, flexures and infants.
- Moderate–potent: trunk, limbs or thicker eczema.
- Use the lowest potency that adequately controls inflammation.
Topical calcineurin inhibitors: tacrolimus or pimecrolimus for sensitive sites, particularly face/flexures, or as steroid-sparing therapy.
Wet-wrap therapy: short-term option for severe or widespread flares, usually with emollient ± topical corticosteroid.
Moderate, Severe and Refractory disease
Phototherapy: narrow-band UVB.
Biologics
- Dupilumab: IL-4/IL-13 pathway inhibitor; monitor conjunctivitis and injection reactions.
- Tralokinumab or lebrikizumab: IL-13 inhibitors.
Oral JAK inhibitors: upadacitinib, abrocitinib or baricitinib, depending on local approval; rapid effect but require infection-risk assessment and laboratory monitoring.
Conventional systemic therapy: ciclosporin, methotrexate, azathioprine or mycophenolate in selected patients.
Continue topical therapy and emollients alongside systemic treatment.
Avoid routine systemic corticosteroids due to adverse effects and rebound flares.
Complications & Prognosis
- Psychological stress
- Side effects of Corticosteroids
- Bacterial Infections
- Atopic dermatitis is a chronic disease with a varying course.
- Approximately 60% of children will have symptom resolution as they enter puberty, but relapse may occur in 50%.
References
- Sidbury R, Alikhan A, Bercovitch L, Cohen DE, Darr JM, Drucker AM, et al. Guidelines of care for the management of atopic dermatitis in adults with topical therapies. J Am Acad Dermatol. 2023;89(1):e1-e20. doi:10.1016/j.jaad.2022.12.029.
- Davis DMR, Drucker AM, Alikhan A, Bercovitch L, Cohen DE, Darr JM, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. J Am Acad Dermatol. 2024;90(2):e43-e56. doi:10.1016/j.jaad.2023.08.102.
- Chu DK, Schneider L, Asiniwasis RN, Boguniewicz M, De Benedetto A, Ellison K, et al. Atopic dermatitis (eczema) guidelines: 2023 AAAAI/ACAAI Joint Task Force on Practice Parameters GRADE- and Institute of Medicine-based recommendations. Ann Allergy Asthma Immunol. 2024;132(3):274-312. doi:10.1016/j.anai.2023.11.009.
- Wollenberg A, Kinberger M, Arents B, Aszodi N, Barbarot S, Bieber T, et al. European Guideline (EuroGuiDerm) on atopic eczema: living update. J Eur Acad Dermatol Venereol. 2025;39(9):1537-1566. doi:10.1111/jdv.20639.
- Goh MSY, Yun JSW, Su JC. Management of atopic dermatitis: a narrative review. Med J Aust. 2022;216(11):587-593. doi:10.5694/mja2.51560.



{kind=link}
Members only discussions coming soon…