Bowel Obstruction


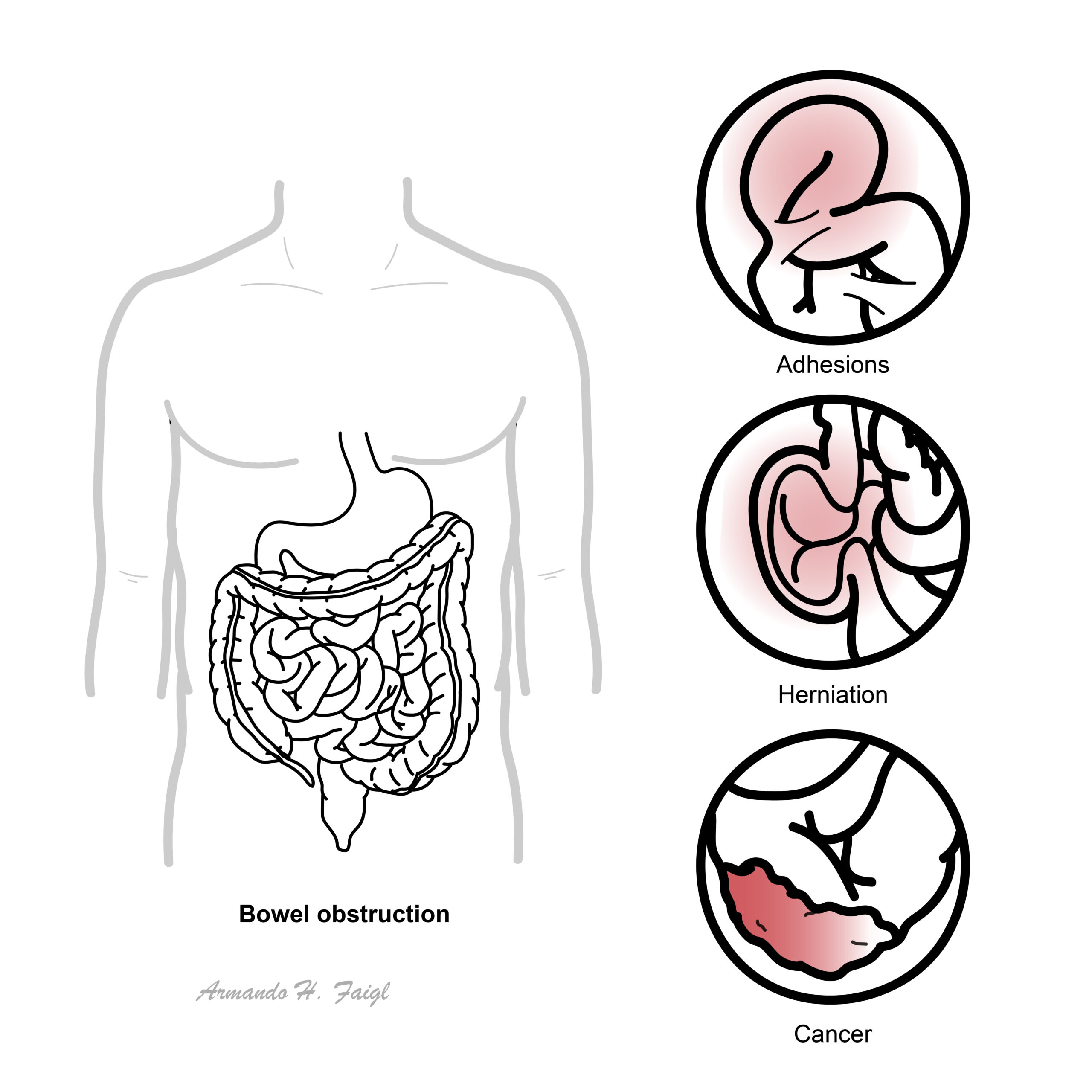
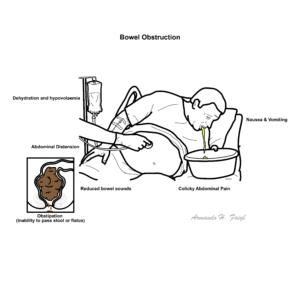
Bowel obstruction is a blockage of intestinal contents, either mechanical (e.g., adhesions, hernias, malignancy) or functional (e.g., ileus), leading to impaired transit, proximal dilation, and downstream complications including ischaemia and perforation if untreated. Key features of bowel obstruction include colicky abdominal pain, distension, nausea with bilious or faeculent vomiting, obstipation, initially high-pitched then absent bowel sounds, and signs of dehydration or hypovolaemia.
Common in postoperative patients, older adults, and individuals with prior abdominal surgeries. Small bowel obstructions are often caused by adhesions; large bowel obstructions frequently result from malignancy or volvulus. Ileus is more common in hospitalized or post-surgical patients. Bowel obstruction is a surgical emergency with high morbidity and mortality if unrecognized.
Cardinal features of intestinal obstruction: vomiting, colicky pain, constipation and distension.
Several categories have been used to classify differences in the various presentations of intestinal obstruction. Ask yourself:
Cardinal features of bowel obstruction?
| Differences in Aetiology between small, large bowel obstruction and ileus1 | |||
| Small Bowel | Large Bowel | Ileus | |
| Main Aetiologies (in order) | 1. Adhesions from previous surgeries 2. Hernia 3. Cancer 4. Strictures secondary to IBD | 1. Malignancy 2. Volvulus 3. Strictures secondary to Diverticulitis and IBD | 1. Post-operative 2. Medication induced 3. Chronic disease |
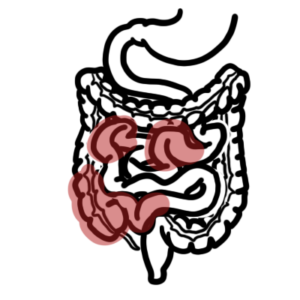
Obstruction or disruption of bowel contents results in a blockade, leading to proximal bowel dilation and distal decompression. This decompression typically occurs over 12–24 hours, during which time small amounts of flatus and faeces may still pass—referred to as a partial obstruction. Continued accumulation of gas and intestinal contents increases intraluminal pressure, resulting in the following sequelae:
Small Bowel | Large bowel | Ileus | |
| Nausea & vomiting | – Early onset – Bilious | – Later onset – Bilious – Progresses to faeculent | Present |
| Abdominal Pain and Distension | – Colicky – slight distention + | – Colicky – Significant distension and earlier onset | Minimal or absent |
| Obstipation (inability to pass flatus or stool) | – Present, however can still pass in initial 12-24hrs of obstruction | Present | + |
| Bowel Sounds on Auscultation | – Initially increased (high pitched) – Later: Reduced or absent (tinkling) | – Initially increased (high pitched) – Later: Reduced or absent (tinkling) | Decreased or absent |
| Physical Exam findings | – Systemic signs: Dehydration and signs of hypovolaemia (dry mucous membranes and hypotension) – Diffuse abdominal tenderness – Abdominal distension – Tympanic percussion DRE: Possible fecal impaction or rectal masses as the source of obstruction | ||
Clinical signs associated with bowel ischaemia (note: these are nonspecific)
Given the urgency of bowel obstructions, prompt imaging and supportive therapy is required as soon as possible before pursuing other investigations.
Imaging
| DIFFERENCE BETWEEN SMALL AND LARGE BOWEL OBSTRUCTION on X-ray | ||
Small Bowel | Large bowel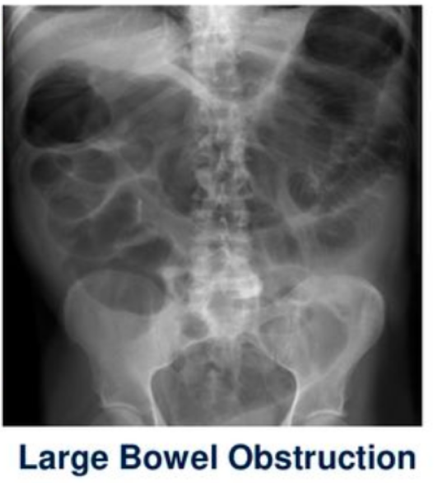 | |
| Location of dilated bowel loops | Central abdomen | Peripheral abdomen |
| Bowel wall pattern | Valvulae conniventes – folds/lines that cross full width of bowel | Haustral folds (lines do not cross entire lumen) |
| Air-fluid levels (Erect film) | Multiple short, “step-ladder” – like air-fluid levels (image from https://litfl.com/axr-interpretation/) | Fewer, longer air-fluid levels |
| Gas and distension pattern (supine) | Proximal distension + no colonic gas | Proximal distension + distal decompression No small bowel air if competent ileocaecal valve |
| Thumbprinting | May be present due to bowel wall oedema/ischaemia image from https://www.radiologymasterclass.co.uk/tutorials/abdo/abdomen_x-ray_abnormalities/pathology_inflammatory_bowel | |
| Pneumoperitoneum (erect/decubitus) | Seen as free air under diaphragm if perforation occurs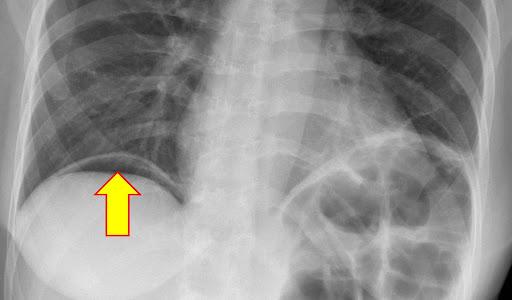 | |
| Side note NORMAL X-RAY DIFFERENCES OF SMALL AND LARGE BOWEL | ||
| Small bowel | Large bowel | |
| Location | Central | Peripheral |
| Content | Fluid and air | Faecal matter |
| Wall Patern | Valvulae conniventes (transverse mucosal folds that cross entire lumen) | Haustral folds (do not cross entire lumen); interspersed with plicae semilunares |
| Size | 3cm diameter | 6cm diameter (caecum 9cm) |
3, 6, 9 Rule
Small intestine 3cmLarge intestine 6cmCaecum 9cm
Any increase in these numbers signify dilatation most likely due to an obstruction.
Laboratory investigations
Additional investigations are done to investigate potential underlying causes or determine the presence of ischaemic changes3
Bowel obstructions can be classified in a variety of ways, such as:
[Pseudo-obstruction refers to intestinal dysmotility syndromes that have signs, symptoms, and the radiologic appearance of obstruction in the absence of a mechanical cause.]
1. Initial Supportive Management (for ALL patients):5
2. Definitive Management (if complications are present):5
Complications
Prognosis
Prognosis varies based on cause and timeliness of intervention. Most mechanical obstructions require surgery if complications arise. Delayed treatment increases risk of ischaemia, sepsis, and death. Functional obstructions (e.g., ileus) typically resolve with supportive care.










Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion