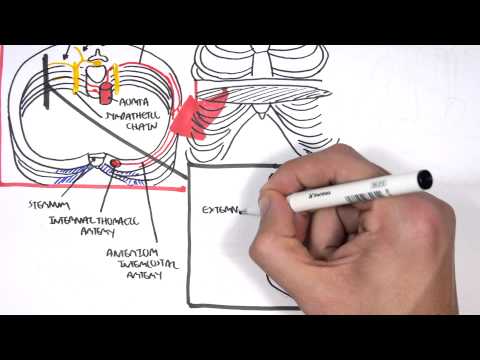
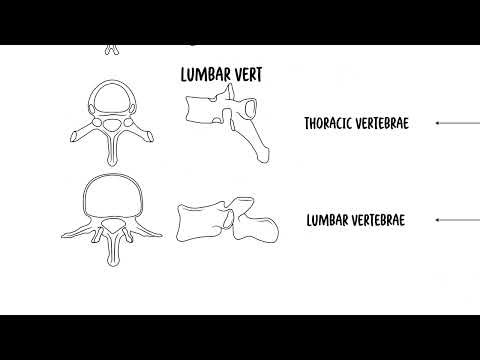
0:00 Hello in this video, we're going to look at anatomy of the thorax. 0:09 So here I'm drawing the rib cage, the thorax area from an anterior view. 0:16 And here at the back is our vertebrae, the thoracic vertebrae. 0:20 We have 12 in total, so T1 all the way to T12. 0:24 And I'm also adding the lumbar one, the lumbar vertebrae number one. 0:29 Starting off the thoracic vertebrae 12, so T12, we have the 12th rib, which is 0:35 a floating 0:36 rib here. 0:38 Here is our clavicle and scapula. 0:42 Now the ribs originate from the vertebrae and connect to the sternum. 0:48 The ribs actually joining to the sternum form college, allowing for the 0:54 expansion of the 0:55 thorax during respiration. 0:58 The sternum itself forms three parts, the manubrium of the sternum, the body of 1:02 the sternum, and 1:03 the zyphoid process of the sternum. 1:07 During the sternum from a side view now, it is important to appreciate an 1:11 important landmark, 1:12 which is marked by the sternal angle between the manubrium and the body of the 1:18 sternum. 1:18 This surface marking is also referred to as the angle of lewy. 1:24 On the side view of the sternum, we can see the insertion points of the ribs. 1:31 Rib one attaches onto the manubrium, rib two to the sternal angle, rib three to 1:36 six to 1:37 the body of the sternum. 1:39 And here is the zyphoid sternal joint. 1:44 And on top here is the clavicular notch, where the clavicle attaches. 1:49 The clavicle and sternum make up the sternoclavicular joint. 1:55 Now as I said, the sternum angle, or the angle of lewy, is an important 1:59 landmark because 2:00 many structures can be found along this angle. 2:05 So if we were to cut straight along in a horizontal plane along this sternum 2:11 angle, we will hit 2:12 and find these things such as the joint between thoracic vertebra IV and V, so 2:22 T45. 2:24 The second rib articulation occurs here. 2:28 We can find the aortic arch, zygus vein as well, entering into the heart. 2:34 We have the ligamentum arteriosus, we have the left recurrent laryngeal nerve, 2:38 we can 2:39 also find the bifurcation of the pulmonary trunk and bifurcation of the trachea 2:46 . 2:46 Now let's talk a bit more about ribs. 2:48 So ribs can be divided into true, false and floating. 2:54 True ribs are also known as the vertebro-costal ribs, which are ribs one to 2:59 seven. 3:00 These are ribs that originate from the vertebra and join to the sternum through 3:05 the costal 3:05 cartlages, then you have false ribs or vertebro-bromco-contral ribs, which are 3:13 ribs 8, 9, 10. 3:15 And these ribs originate from the vertebra and attach to the sternum by joining 3:21 to the 3:22 cartlages of ribs six and seven. 3:27 Finally you have floating ribs or the vertebro-rib free ribs, which are ribs 11 3:33 and 12. 3:34 These are the ribs that originate from the vertebra but don't attach anywhere. 3:40 Our ribs can also be divided into typical and atypical. 3:45 Typical ribs are ribs with similar features, typical features, and these ribs 3:50 are ribs three 3:51 to nine. 3:53 Atypical ribs are different from each other and other ribs, and our ribs one, 3:59 ribs two and 4:00 ribs ten to twelve. 4:05 Okay now let's look at a posterior view of the thoracic, the thorax, the rib 4:11 cage. 4:11 Here I'm drawing the vertebrae again, the clavicle and scapula, and here are 4:17 the ribs 4:17 one to twelve. 4:21 Here is the scapula clavicle, and here is the lumba vertebra one. 4:27 Let's talk about the vertebra, the vertebrae quickly, just for a quick recap. 4:32 We are looking at a vertebrae from a superior view. 4:37 This is T1, and here is the body. 4:40 The vertebral foramen is where the spinal nerve goes through, spinal cord sorry 4:45 goes 4:45 through. 4:46 The peduncle, we have the transverse process, and then we have the spinous 4:48 process, which 4:49 we can actually feel when we palpate along the spine. 4:54 So here is the thoracic vertebra six, T6, which is very similar to the previous 5:01 vertebrae, 5:03 but something else that is very important to introduce is the facets where ribs 5:08 articulate, 5:09 and this is specifically for the thoracic vertebrae, because they have ribs 5:15 coming off 5:16 them. 5:18 Finally we have T12, very much the same with other thoracic vertebrae. 5:24 But T12 especially becomes bigger when we go towards the lumba vertebrae. 5:29 Okay, next let's look at where organs and other things lie in respect to the 5:34 thoracic 5:35 cavity. 5:37 So this is an anterior view again. 5:40 Now roughly along the fifth rib is where the diaphragm sits. 5:48 The landmarks to remember is the mid-clavicular, which is essentially the site 5:55 from, if we 5:56 draw a line from the middle of the clavicle down, so this is mid-clavicular. 6:00 There is also a mid-scapula, which is a landmark at the back, the middle of the 6:06 scapula. 6:07 The mid-exidery is the landmark for the lateral aspects of the thorax along the 6:11 armpits. 6:12 These landmarks are important to know because of several reasons, one of which 6:16 is to help 6:17 identify where the lung sits in respect to the thoracic cavity and also the ple 6:24 ural flow 6:25 or the pleural itself. 6:28 So next let's talk about the surface landmarks of the lung itself and also the 6:37 parietal pleural. 6:39 So again the pleural is essentially a membrane that covers our lungs. 6:47 The pleural can be divided into parietal and visceral pleural. 6:50 Visceral pleural is the one that covers all our lungs and the parietal pleural 6:56 is the layer 6:57 above it. 7:01 So the margins of the lung, mid-clavicular, it goes to the sixth rib, mid-ex 7:06 idery to the 7:07 eighth rib, and mid-scapula, the tenth rib. 7:12 So the margins of the lung, mid-clavicular, it goes to the sixth rib, mid-ex 7:18 idery to the 7:19 eighth rib, and mid-scapula, the tenth rib. 7:23 So if I were to draw it out on this diagram, it would be something like this. 7:27 So mid-exidery, it goes to the eighth rib, the lung, and then mid-clavicular, 7:33 it goes, 7:34 it is on the sixth rib, and at the back, mid-scapula, the lung margin is on the 7:38 tenth rib. 7:41 The pleural here in blue goes further down. 7:45 You essentially add two to find the margins of the pleural. 7:50 So mid-exidery, it's at rib 10, mid-clavicular, it's the rib 8. 7:54 So margin of the pleural, mid-clavicular, plus 2 is 8, mid-exidery is 10, and 8:03 mid-scapula 8:05 is 12. 8:06 I hope that makes sense. 8:08 Now the margins of the lung and pleural, on the left side of the thorax, is 8:14 slightly different. 8:16 Because of where the heart is situated, the heart sits somewhere here. 8:22 Because remember, the aorta goes up and it's behind the sternal angle. 8:27 Again here in red, I'm drawing the margins of the lung. 8:31 The margins of the lung on the left side, instead of being mid-clavicular on 8:35 the sixth 8:36 rib, it is mid-clavicular on the fourth rib. 8:41 It goes down to being mid-exidery on the eighth rib, then everything else is 8:46 the same. 8:47 So it's just where the heart is that makes the left and right lung margins and 8:52 pleural, 8:53 pleural margins slightly different. 8:57 Just to finish off this diagram, the liver, or most of the liver can be found 9:02 under our 9:02 ribs for protection. 9:07 Now let's look at what problems can occur in the thoracic cavity. 9:12 Let's look at a pulmonary collapse, a result of a pneumothorax. 9:19 A collapsed lung is also referred to as adelectasis. 9:23 So normally here is our lung, surrounding our lung is the visceral pleural, 9:28 then our 9:29 parietal pleural. 9:31 In between the visceral and parietal pleural, we have the pleural cavity, which 9:34 helps lubricate 9:35 the layers and keep them stuck together. 9:39 And here is the cardiac area where the heart sits. 9:43 Remember air moves in and out as we inhale and exhale. 9:48 A pneumothorax can occur because of something external puncturing the pleural 9:52 layer, the 9:53 parietal layer, resulting in air moving into the pleural cavity. 9:58 This results in air filling the parietal pleural cavity and forcing the lungs 10:03 to deflate essentially. 10:05 So injury results in puncturing of the parietal pleural. 10:12 The punctured parietal pleural allows air to enter the pleural cavity. 10:17 Air entering the pleural cavity compresses the lung resulting in a collapsed 10:21 lung. 10:22 However, what we looked at was pneumothorax occurring as a result of an 10:26 external trauma. 10:27 What is important to know is that a pneumothorax can also occur when the lung 10:31 and visceral 10:32 pleural is damaged, resulting in air filling the pleural cavity, causing a 10:38 pneumothorax 10:38 as well. 10:40 This can be seen in lung diseases such as COPD, or in tall, skinny people who 10:44 have predisposition 10:45 for spontaneous pneumothorax. 10:48 So I hope you enjoyed this video, thank you for watching.