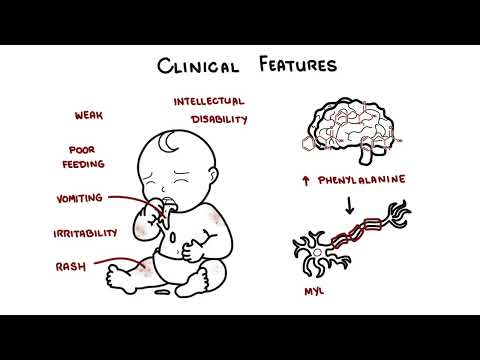
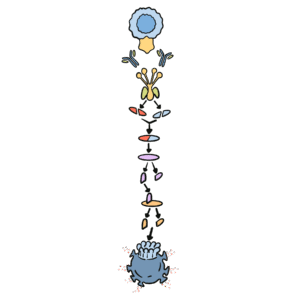
0:00 Today, we will be discussing a rare but significant chromosomal disorder known 0:09 as Edward's syndrome 0:10 or trisomy 18, and it was first described by geneticist John Hilton Edwards in 0:17 1960. 0:18 Edward's syndrome is a genetic disorder affecting approximately 1 in 5,000 to 6 0:22 ,000 live births 0:23 caused by the presence of an extra chromosome 18. 0:27 It affects females more than men, a three to one ratio. 0:30 Now, in a typical human cell, there are 23 pairs of chromosomes. 0:34 However, in Edward's syndrome, there is a third copy of a chromosome 18, and 0:39 this additional 0:40 genetic material disrupts normal development, leading to a variety of severe 0:44 physical and 0:45 intellectual disabilities. 0:47 The exact cause of trisomy 18 is usually a random error in cell division called 0:53 non-disjunction, 0:55 which results in an extra copy of chromosome 18. 0:59 Although this error can occur in any pregnancy, the risk increases with 1:04 maternal age. 1:05 Women over the age of 35 have a higher likelihood of having a child with Edward 1:13 's syndrome. 1:15 Let's revise some genetics now to understand how this all happens. 1:20 Typically, a person has 46 chromosomes or 23 pairs of chromosomes that make up 1:26 each cell. 1:27 You get 23 from mum, and 23 chromosomes from dad. 1:32 Let's see how the mother's egg and the father's sperm are created and how they 1:37 form a new embryo 1:38 with 46 chromosomes. 1:41 To form the mother's egg or father's sperm, the process is called meiosis. 1:45 Here we are looking at the mother specifically. 1:48 The mother has 46 chromosomes. 1:51 These chromosomes first will duplicate, then divide to split the 46 chromosomes 2:00 evenly, 2:01 forming two cells with 23 duplicated chromosomes. 2:06 In the second stage of meiosis, these actually will divide again, splitting the 2:12 duplicated 2:12 chromosomes, resulting in sex cells with 23 single chromosomes each, so no 2:20 longer duplicated. 2:22 These are the sex cells, and this is the female egg. 2:26 The father's sperm, which also has 23 chromosomes, will fertilize the egg, and 2:30 the combination 2:30 forms an embryo with 46 chromosomes, 23 from the mother and 23 from the father. 2:38 These with Edward syndrome have an extra copy of one of these chromosome, 2:43 chromosome 18, 2:44 and there are three ways this could happen, and so three types of Edward 2:48 syndrome, trisomy 2:50 18 non-disjunction, which is the most common, 90%. 2:55 Translocation involving chromosome 18, this is also known as partial trisomy 18 3:00 , and then 3:01 trisomy 18-mossacism. 3:08 The great majority of babies with Edward syndrome have trisomy 18, usually due 3:12 to non-disjunction, 3:14 usually during maternal oogenesis, when the female egg is being made through me 3:20 iosis. 3:21 As you can see in this example, a diagram of maternal oogenesis, meiosis 1 3:27 occurs normally, 3:29 but in meiosis 2, one egg can have an extra chromosome 18 making 24 instead of 3:36 23 chromosomes, 3:38 and this is a result of non-disjunction. 3:42 The sperm with 23 chromosomes then fertilizes the egg with 24 chromosomes 3:47 making 47 chromosomes. 3:49 The extra chromosome is chromosome 18. 3:52 The fertilized egg, the baby, has three separate copies of chromosome 18, and 3:57 so this baby, 3:58 when it cells begin to divide and the baby grows, each of these cells will have 4:02 three 4:03 copies of chromosome 18. 4:05 Again, about 90% of Edward syndrome patients or cases have a complete trisomy 4:17 18. 4:18 Then you have translocation involving chromosome 18, also known as partial tris 4:23 omy 18, and 4:24 this type is where an extra part or a whole extra chromosome 18 is present. 4:29 However, the extra chromosome is attached or translocated to a different 4:36 chromosome, rather 4:37 than being a separate chromosome 18. 4:39 An example is translocation between chromosome 15 and 18. 4:43 Let's just say the mother is a carrier for this translocation. 4:48 As you can see, the mother has technically two chromosome 15 and two chromosome 4:54 18. 4:54 We can compare this to a normal pair of chromosome 18 and chromosome 15. 5:01 During sex cell production, the meiosis, this particular cell, as it divides, 5:05 can achieve 5:06 different outcomes in terms of eggs. 5:09 One egg in particular can result in two chromosome 18s. 5:14 And so, when a sperm containing 23 chromosomes fertilizes this egg, the new 5:21 cell and baby 5:22 will have three copies of chromosome 18, hence trisomy 18, or partial trisomy 5:28 18 to be exact. 5:35 The final is trisomy 18, Mosaicism. 5:39 Mosaic Edward Syndrome is caused by a random event shortly after the egg and 5:45 sperm join 5:46 together. 5:47 So, nothing to do with meiosis. 5:49 When cells are dividing, this is called mitosis, and some cells can receive an 5:53 extra copy of 5:54 chromosome 18, others do not. 5:58 People with Mosaic Edward Syndrome have some cells with two and some cells with 6:02 three copies 6:03 of chromosome 18. 6:08 And so, these different mechanisms of getting three copies of chromosome 18, 6:13 whatever the 6:13 way, will result in the clinical features of Edward Syndrome. 6:18 Edward Syndrome is associated with multiple congenital anomalies. 6:22 Common clinical features include craniofacial abnormalities, such as a small 6:27 head, micro 6:27 carefully, prominent occiput, low set ears, a small jaw, micro nathia, and a 6:33 cleft lip 6:34 or palate. 6:36 Very important are hand abnormalities. 6:38 They usually have clenched fists with overlapping fingers and underdeveloped 6:42 thumbs are these 6:43 classic findings. 6:45 Cardiac defect is also very common. 6:47 Over 90% of infants are born with a congenital heart defect, such as vent 6:51 ricular septal defect 6:53 or patent ductus arteriosus. 6:56 Other abnormalities include rocker bottom feet, feet that are round at the 7:00 bottom, as though 7:01 they can rock, a narrow pelvis, and growth restriction. 7:07 Edward Syndrome shares some features to try some E13, also known as pato 7:11 syndrome, which 7:12 I'll discuss in a separate video. 7:21 Edward Syndrome can often be detected during pregnancy through routine 7:25 ultrasound screening, 7:26 which may reveal abnormalities such as a small size for gestational age or 7:30 heart defects, 7:31 after you try and growth restriction associated with polyhydramnios and clench 7:36 fist sign is 7:37 a highly suggestive sign of Edward Syndrome. 7:40 Definitive diagnosis however is made through prenatal tests such as amnocent 7:46 esis or chorionic 7:47 vellus sampling, where a carrier type analysis of the fluid or sample of the ch 7:55 orion will 7:56 identify the extra chromosome 18. 8:04 Now what about prognosis and life expectancy? 8:07 Edward Syndrome is associated with a high rate of stillbirths and infant 8:11 mortality. 8:12 The majority of prenatal diagnosed cases of trisomy 18 die neutral. 8:17 Unfortunately only 5 to 10% of affected children survive beyond the first year. 8:22 Those who do survive often have profound intellectual disabilities and ongoing 8:25 medical needs. 8:28 The severity of symptoms and life expectancy depends on whether the child has 8:32 full, mistake 8:33 or partial trisomy 18. 8:40 There's no cure for Edward Syndrome and treatment focuses on managing symptoms 8:43 and providing 8:43 supportive care. 8:45 Due to complex medical needs of these infants, a multidisciplinary team 8:49 approaches essential 8:50 and this includes a pediatric specialist, cardiologist, geneticist and palli 8:54 ative care specialist. 9:01 So in summary, Edward Syndrome is a complex condition with significant medical 9:05 challenges, 9:06 early diagnosis, appropriate medical care and support for found is our critical 9:09 components 9:09 in managing this disorder. 9:11 It is caused by trisomy 18, most commonly through non-disjunction. 9:17 Thank you. 9:20 [BLANK_AUDIO]