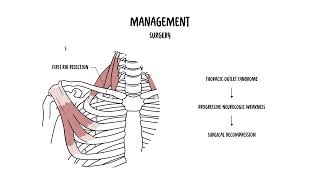
0:00 Thoracic Outlet Syndrome refers to a group of disorders caused by compression 0:17 of the 0:17 brachial plexus, the subclavian artery or subclavian vein, in the thoracic 0:23 outlet, which 0:24 is a tunnel that runs from the neck to the upper arm. And atomically, the thor 0:30 acic outlet 0:31 is bordered by anteriorly the anterior scalene muscles, posteriorly the middle 0:36 scalene muscles, 0:38 inferiorly the first rib. This is the area where most of the compression occurs 0:51 . There 0:52 are three main types of thoracic outlet syndrome classified based on the 0:56 structure that is 0:57 compressed. So you have neurogenic venous or arterial. In neurogenic thoracic 1:04 outlet 1:04 syndrome, this is the most common, up to 90%. And here you get some form of 1:11 compression 1:12 of the brachial plexus and obviously causing some sort of neuropathy. Venus 1:17 thoracic outlet 1:18 syndrome affects the subclavian vein. Artorial thoracic outlet syndrome is the 1:22 least common 1:23 but most serious because you're compressing the artery, specifically the subcl 1:33 avian artery. 1:35 So let's look at the mechanisms of thoracic outlet obstruction. Thoracic outlet 1:41 syndrome 1:41 occurs usually secondary to compression of the subclavian artery, vein, and br 1:46 achial plexus 1:47 at the level of the thoracic outlet. The thoracic outlet consists of three main 1:52 passage ways, 1:54 through which the neurovascular structures travel from the neck to the upper 1:58 limb. Compression 1:59 at any one of these sites can contribute to thoracic outlet syndrome. The three 2:04 main 2:04 passage ways include the interscaling triangle, the cost of claviculate space, 2:11 and the subcorachoid 2:13 or retropectoralis minor space. The neurovascular bundle can be compressed or 2:20 irritated at any 2:22 of these structures or any of these points. So let's take a look at each of 2:31 these areas. 2:34 The first is the interscaling triangle. The interscaling triangle is the first 2:40 narrowing 2:41 area and is the most proximal. Compression causing thoracic outlet syndrome 2:47 most often 2:48 occurs at this point, and this is the area that was introduced at the beginning 2:53 of the 2:54 video. Now this triangle is bordered anteriorly, again, by the anterior scaling 3:00 muscles, posteriorly 3:01 by the middle scaling muscle and inferiorly by the first rib. The brachial plex 3:08 us and the 3:08 subclavium artery pass through the space. Anatomical variations, such as the 3:14 presence 3:15 of the scaling minimus muscle or overlapping insertion of the anterior and 3:19 middle scalines 3:20 on the first rib, can reduce the available space and contribute to the 3:25 compression of 3:26 any of these structures, the brachial plexus or the artery. 3:34 The second passageway of where the thoracic outlet obstruction can occur is 3:40 called the 3:41 costoclavicular space or triangle, and is bordered by the superiorly by the 3:46 middle third 3:47 of the clavicle, so by the clavicle superiorly, inferiorly by the first rib, 3:52 posteriorly and 3:53 medially by the costoclavicular ligament. Now here, the subclavian vein, the 4:00 subclavian 4:01 artery and brachial plexus pass through. Compression of these structures can 4:07 occur as a result 4:08 of congenital abnormalities, trauma to the first rib or clavical fractures. 4:16 Structural 4:16 changes in the subclavian muscles or the costocara coit ligament can also 4:24 contribute to compression. 4:31 Then, we have the subcora coit or the retropectoralis minor space. The final 4:38 passageway 4:40 of thoracic outlet obstruction lies beneath the cora coit process, just under 4:46 the tendon 4:47 of the pectoralis minor. It is bordered superiorly by the cora coit process, 4:47 anteriorly by the 4:56 pectoralis minor muscle, and posteriorly by ribs 2-4. Shortening or tightness 5:03 of the pectoralis 5:05 minor can lead to narrowing of this space, particularly during hyperabduction 5:13 of the shoulder, resulting 5:15 in neurovascular compression. So, those are the three sites of where thoracic 5:22 outlet obstruction 5:24 can occur. So, what are some other contributing factors to developing thoracic 5:33 outlet syndrome? 5:34 Well, there are several congenital or acquired anatomical abnormalities that 5:40 can further compromise 5:41 the thoracic outlet. And this includes the presence of a cervical rib, congen 5:48 ital soft tissue 5:49 abnormalities, a long C7 transverse process, fibrous bands or muscular 5:55 anomalies, such 5:57 as a broad-scaling attachment or hypertrophyid scalenes, clavicular hypo-mob 6:03 ility, scoliosis 6:05 or elevated scapula. And then, obviously, there can be some functionally 6:09 acquired anatomical 6:11 change. So, thoracic outlet syndrome is relatively uncommon, and its exact 6:20 prevalence is difficult 6:21 to determine due to inconsistent diagnostic criteria and under-reporting. Thor 6:26 acic outlet 6:26 syndrome is more frequently diagnosed in women. This is believed to be due to 6:29 anatomical and 6:31 physiological differences, such as narrower thoracic outlet, less developed dem 6:36 uscular 6:36 shoulders, greater breast tissue leading to shoulder depression, and a lower 6:43 position 6:43 of the sternum, which may alter the angle between the scalene muscles and 6:47 predispose 6:48 women to compression. Most cases are diagnosed between ages of 22 and 50, and 6:55 the condition 6:55 is rarely seen in children. About 95% of thoracic outlet syndrome cases, as 7:00 mentioned, are neurogenic, 7:02 involving the brachial plexus. So, what are the clinical features? Well, there 7:11 are three 7:11 main types of thoracic outlet syndrome, as mentioned. So, in neurogenic thorac 7:17 ic outlet 7:18 syndrome, which is the most common, compression of the brachial plexus can lead 7:22 to numbness, 7:22 tingling, weakness in the arm and ham, in a nonspecific dermatonal distribution 7:28 . Venus 7:29 thoracic outlet syndrome affects the subclavian vein. And so, the symptoms can 7:33 include arm 7:34 swelling, cyanosis, heaviness, especially after activity, and it may be 7:39 associated with 7:41 effort thrombosis, something called "pagit-shroita syndrome." Arterial thoracic 7:49 outlet 7:49 syndrome is compression of the subclavian artery. This is by far the rarest, 7:54 but symptoms 7:55 include cool hands, pallor, decreased pulse, and ischemic pain, so pain or with 8:01 activity. 8:03 One examination, you know, it's important to inspect the general anatomy of the 8:15 shoulder 8:15 in the upper limb, but also to assess muscle power and perform a neuro-logical 8:19 examination. 8:20 There are special tests to do, and these tests aim to reproduce the patient's 8:25 symptoms by 8:25 stressing the neuro-vascular structures within the thoracic outlet. They are 8:29 not diagnostic 8:31 on their own, but may support clinical suspicion when positive. You have this 8:36 thing called the 8:36 AdSense test. This is where you have loss of radial pulse with head turning to 8:42 the affected side, 8:44 extended with shoulders, also extended, as shown. The roost test is when you 8:51 have the arms elevated. 8:53 Both arms are raised to 90 degrees, abduction, and external rotation. The 8:59 patient is asked to 9:00 open and close their hands repeatedly, like clenching fists, for three minutes, 9:04 and symptoms can 9:07 recur in thoracic outlet syndrome. 9:13 Rites test, also known as hyper-abduction test, stresses the sub-corachoid 9:21 space, 9:22 where the pectoralis minor can compress the neuro-vascular bundle. This is in 9:27 shoulder abduction, 9:29 hyper-abduction. A positive test suggests compression of the brachial plexus 9:34 and/or auxiliary artery in this space. The patient sits or stands while the 9:39 examiner palpates the 9:40 radial pulse. The arm is then abducted and externally rotated overhead, held 9:46 for one to two minutes 9:47 often, performed on both sides for comparison. Then you have Eden's test. It is 9:53 also known as 9:54 the military brace test. It is designed to test for the costo-clavicular form 9:59 of thoracic outlet 10:00 syndrome. The examiner palpates the radial pulse at the wrist and asks the 10:04 patient to stand, 10:05 push the chest out, and pull the shoulders back as if standing at military 10:11 attention. 10:12 A positive finding is a weakening of the strength of the radial pulse, 10:16 indicating 10:16 compression of the sub-clavian artery in the costo-clavicular space. 10:27 As mentioned, these examinations are not diagnostic. Investigations are 10:31 important, 10:31 including nerve conduction studies, or EMG. This helps confirm urogenic thorac 10:37 ic outlet syndrome, 10:38 and may show reduced ulna-sensory and motor response. Chest X-ray, 10:43 candid-text cervical rib or other bony anomalies, MRI and MRI visualizes soft 10:48 tissue structure, 10:49 scaling muscles, brachial plexus, assesses vascular compression. CT angiogram 10:56 evaluates arterial or 10:57 venous obstruction. Doppler ultrasound detects dynamic vascular compression, 11:02 especially with 11:03 positional changes. So what's the management of thoracic outlet syndrome? Well, 11:13 typically, 11:14 everything is conservative first line. Physical therapy, such as postural 11:18 corrections, strengthening 11:19 of the shoulder girdle muscles, stretching of scaling and pectoralis minor 11:23 muscles, 11:24 pain control if there is pain, anti-inflammatories or muscle relaxants, 11:29 lifestyle modifications, avoid overhead activities and heavy lifting, ergonomic 11:34 adjustments, weight loss, 11:36 if contributing to the symptom. There are interventional options such as 11:45 botulinum toxin injections, so Botox into the scaling or pectoralis minor. This 11:52 provides 11:53 temporarily symptom relief sometimes. Scaling muscle blocks can be diagnostic 11:57 and therapeutic. 12:04 Surgery is obviously last line. When acute or sub-acute progressive neurologic 12:10 weakness occurs, 12:11 secondary to thoracic outlet syndrome surgery is usually needed, surgical 12:15 decompression. 12:16 The surgical approach is determined by the major site of compression, where it 12:21 is. 12:21 The first rib could be contributing. So first rib resection, for example, with 12:26 scale inectomy is the most common operation of choice for surgical decomp 12:32 ression. 12:33 So in summary, thoracic outlet syndrome is a group of disorders where you get 12:40 compression 12:40 of the brachial plexus, sub-clavian artery or sub-clavian vein in the thoracic 12:45 outlet, 12:46 and there are three common sites where obstruction can occur, the most common 12:51 being within the 12:52 interscaling muscles. Thank you for watching.