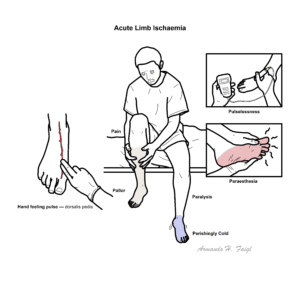
Acute Limb Ischaemia


Acute limb ischaemia refers to any sudden decrease in limb perfusion that causes a potential threat to viability. It is associated with pain, motor and sensory loss, and cold sensation. It affects one in about 6000 of the population1 and is more common in the lower limb, with less than 17% of cases affecting the upper limb4. If left untreated, it can lead to limb loss or even death3.
Acute limb ischaemia is defined by a rapid drop in arterial blood flow resulting in cessation of nutrient and oxygen delivery to the tissues.
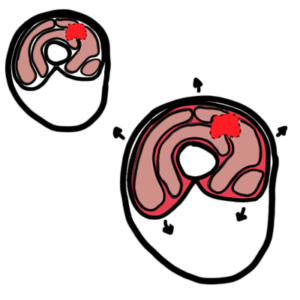
Compartment syndrome is a complication that occurs when there is an increase in pressure in a closed muscle compartment leading to compression of blood vessels and nerves, causing swelling, tightness and pain.
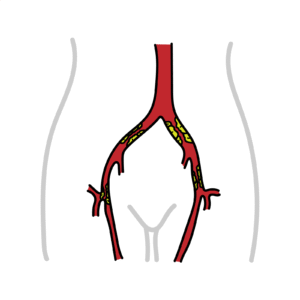
Acute thrombosis in a vessel with preexisting atherosclerosis (60% of cases):
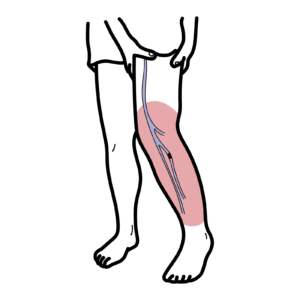
Emboli (30% of cases)
Less common
Sudden onset limb ischaemia in a previously normal limb suggests embolism (often cardiac source, e.g. AF) where as gradual onset, collaterals present → more likely thrombosis on pre-existing PAD.
Virchow’s triad: hypercoagulability, blood flow stasis, endothelial injury – leads to increased risk of thrombosis.
Atrial fibrillation is an atrial arrhythmia that causes impaired contraction of atria leading to blood stasis in the atrium. A clot can form and travel to an artery in the limbs, obstructing blood flow and causing ischaemia.
Arterial occlusion causes sudden cessation in blood flow and nutrient and oxygen delivery to tissues. This leads to the tissue relying on anaerobic instead of aerobic metabolism. Anaerobic metabolism produces lactate, which increases the acidity in affected tissue, causing muscle injury. This eventually leads to depletion of ATP and leakage of free calcium, which causes skeletal muscle fiber necrosis.4
Virchow’s triad – set of 3 factors that contribute to thrombosis, presence of any of the elements increases the risk of acute limb ischaemia:
Divided into 3 classes based on Rutherford criteria:
| TABLE 1. RUTHERFORD CLASSIFICATION OF ACUTE LIMB ISCHEMIA | |||
| Rutherford Class | Sensory Impairment | Motor Impairment | Doppler Signals |
| Class 1 (No immediate threat) | None | None | Arterial: audible Venous: audible |
| Class 2a (Marginally threatened) | Minimal | None | Arterial: audible Venous: audible |
| Class 2b (Immediately threatened) | Involves forefoot with possible rest pain | Mild to moderate | Arterial: absent Venous: present |
| Class 3 (Irreversible ischemia) | Insensate | Severe, rigorous | Arterial: absent Venous: absent |
| Adapted from Gunawansa N. Atraumatic acute limb ischemia: clinical presentation, classification, assessment and management – a review. Int J Vasc Surg Med. 2017;3:046-052. doi: 10.17352/2455-5452.000029 | |||
The most common symptoms are the 6 Ps:
Clinical examination
General inspection: findings change as damage to tissue becomes more prominent, from least to most severe:
Acute limb ischaemia can have a vague presentation, such as mild pain, making the list of potential diagnosis very broad.
Diagnosis
Investigations are performed only if they do not delay urgent vascularisation.
Bedside:
Bloods:
Imaging:
Don’t delay revascularisation for imaging if the limb is immediately threatened.
Creatine kinase (CK) is an enzyme found in the heart, brain and skeletal muscles. It helps produce energy and is released when the tissue is damaged. Higher levels of CK in the blood indicate a higher degree of injury.
Start with an A-E assessment to determine if patient is stable or unstable
Resuscitate if necessary:
1. Give unfractionated heparin to all patients if there are no contraindications (eg. aortic dissection, multiple traumas, head injury) (1)
2. Early vascular consult and confirmatory imaging
Unfractionated heparin is an anticoagulant that is commonly used in patients with venous thromboembolism and cardiovascular disease. Mechanism of action: binds to antithrombin III enhancing its activity, which in turn deactivates factors IIa (thrombin) and Xa. Side effects: the most common is bleeding. Unfractionated heparin can be reversed with protamine sulfate.
3. Perform a limb vitality assessment using examination and urgent Doppler (1,4):
| Examination and doppler | Suggests | Definitive treatment |
| Normal examination Doppler – arterial and venous flow both audible | Viable | Conservative management, usually with anticoagulation |
| Sensory loss in toes, intact motor Doppler – arterial flow may be absent | Marginally threatened | Salvageable with revascularisation |
| Sensory + motor loss Doppler – absent arterial flow | Immediately threatened | Requires urgent revascularisation Fasciotomy (if compartment syndrome suspected) |
| Fixed mottling, hard muscles Doppler – absent arterial and venous flow | Irreversible ischaemia | Amputation likely |
Consider fasciotomy if delayed revascularisation → compartment syndrome risk.
Fasciotomy is a surgical procedure where the fascia (connective tissue covering various organs, including muscles) is cut open to relieve pressure.
Thrombolysis is the use of medication to break down clots. It is used in ischaemia, pulmonary embolism and myocardial infarction. Common medications are urokinase and drugs ending with the suffix -plase (eg. alteplase). Mechanism of action: convert plasminogen to plasmin, which initiates breakdown of fibrin.
Angioplasty is a procedure used to dilate narrow arteries. A catheter is placed in the vessel and a balloon is inflated at the point of narrowing causing the vessel lumen to dilate. A stent is often left in place to prevent recurrent narrowing.
Embolectomy is a surgical procedure used to remove an embolus (blood clot) from an artery. A balloon catheter is inserted inside the artery and the balloon is inflated distal to the embolus, the balloon is then retrieved out of the artery together with the embolus.
Reperfusion injury can occur when blood supply is restored in tissue that has been deprived of oxygen, which causes release of free radicals, oxidative stress and inflammation. This can lead to swelling and cell death.
The mortality and amputation rates depend on the type of treatment received, presence of comorbidities and stage of ischaemia. 7
The in-hospital mortality ranges between 10-20%.5














Discussion