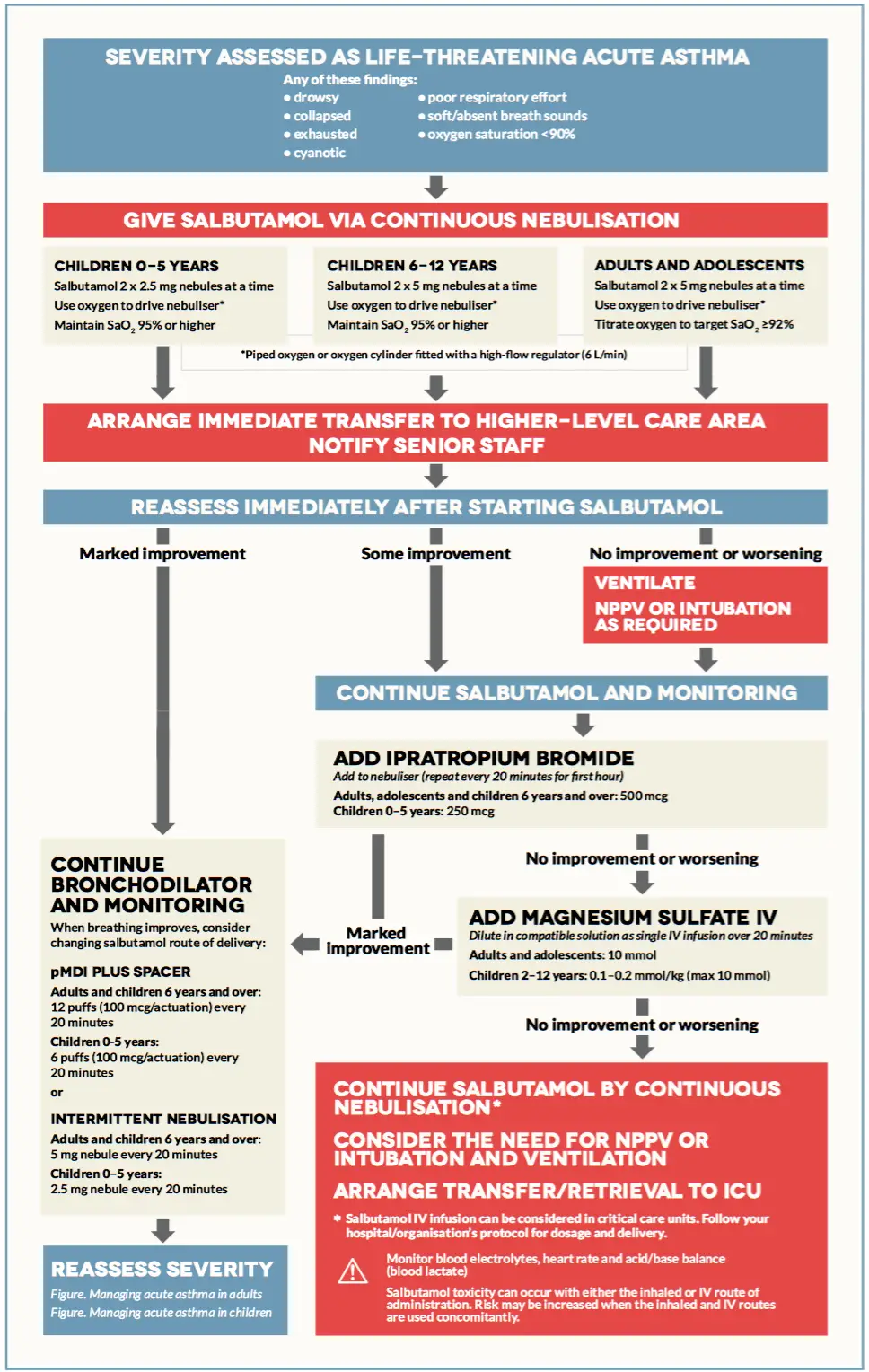
If not responding to any treatment during the 1 hour after bronchodilator, immediate transfer to high level care → move to life-threatening management.
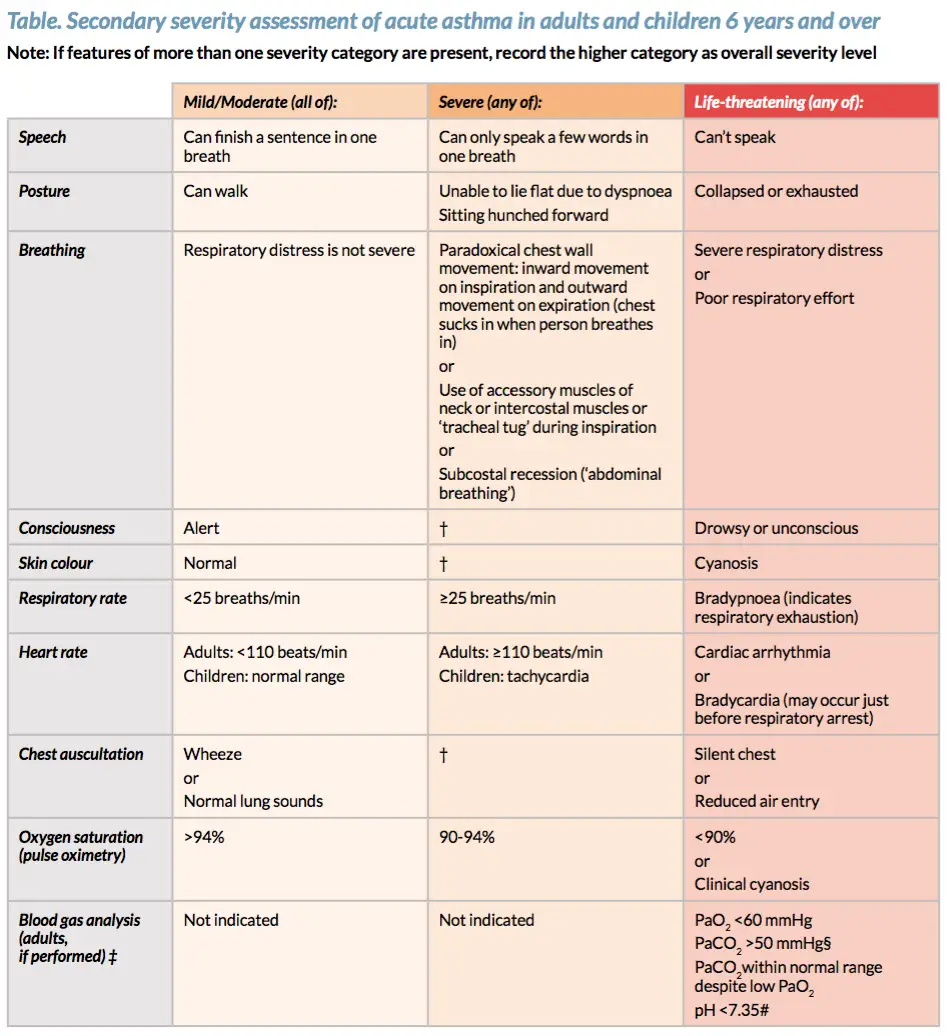
Mneumonic CHEST for life-threatening asthma: Cynosis, Hypotension and Hypoxia (pO2 <90%), Exhaustion, Silent chest, Tachycardia and Threatening PEF < 33% best or predicted (in those >5yrs old).
Treatment
β-agonist (Salbutamol via continous nebulisation)
Anticholinergic – Ippatropium Bromide
Steroids (the earlier given in an attack, the better the outcome)
IV salbutamol
IV magnesium sulphate immediated if very severe
IV aminophylline some patients may respons, give if poor response to intitial therapy
+/- Intubation and ventilation
IV fluids patients are often dehydrated
Antibiotics only if an infection caused exacerbation
Indications for assisted ventilation in asthma
Coma
Respiratory arrest
Exhaustion
Deteriorating ABG
Mneumonic O-SHIT-MI for the management of Severe/Life-threatening asthma: Oxygen, Salbutamol, Hydrocortisone (Prednisolone), Ippatropium bromide, Theophylline, Magnesium sulphate, Intubation and ventilation.
Image from Australian asthma handbook
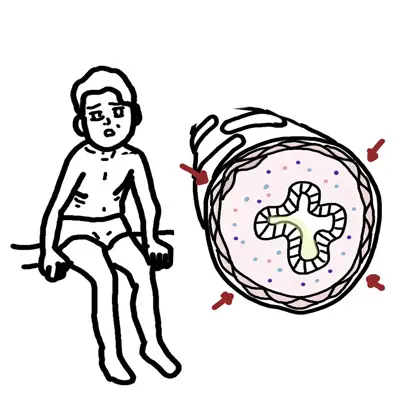
Pathogenesis Asthma Exacerbations
Airway obstruction occurs due to a combination of:
Long-term uncontrolled asthma can lead to air trapping and asthma exacerbations through what is called dynamic hyperinflation.
Airflow obstruction → Slow expiratory airflow and incomplete gas exhalation dynamic hyperinflation → Patient takes next breath → Gas becomes trapped in alveoli
Gas becomes trapped in alveoli until the alveoli can not hold any more gas and exhaled volume = inhaled volume → Equilibrium
Mild asthma
Only most severely obstructed airways collapse
Collapsed airways with air trapping results in:
Decreased expiratory reserve volume
Increased residual volume
As asthma gets more severe
Expiratory reserve diminishes and this results in profound dyspnoea

















Discussion