

Polyarteritis Nodosa

Overview
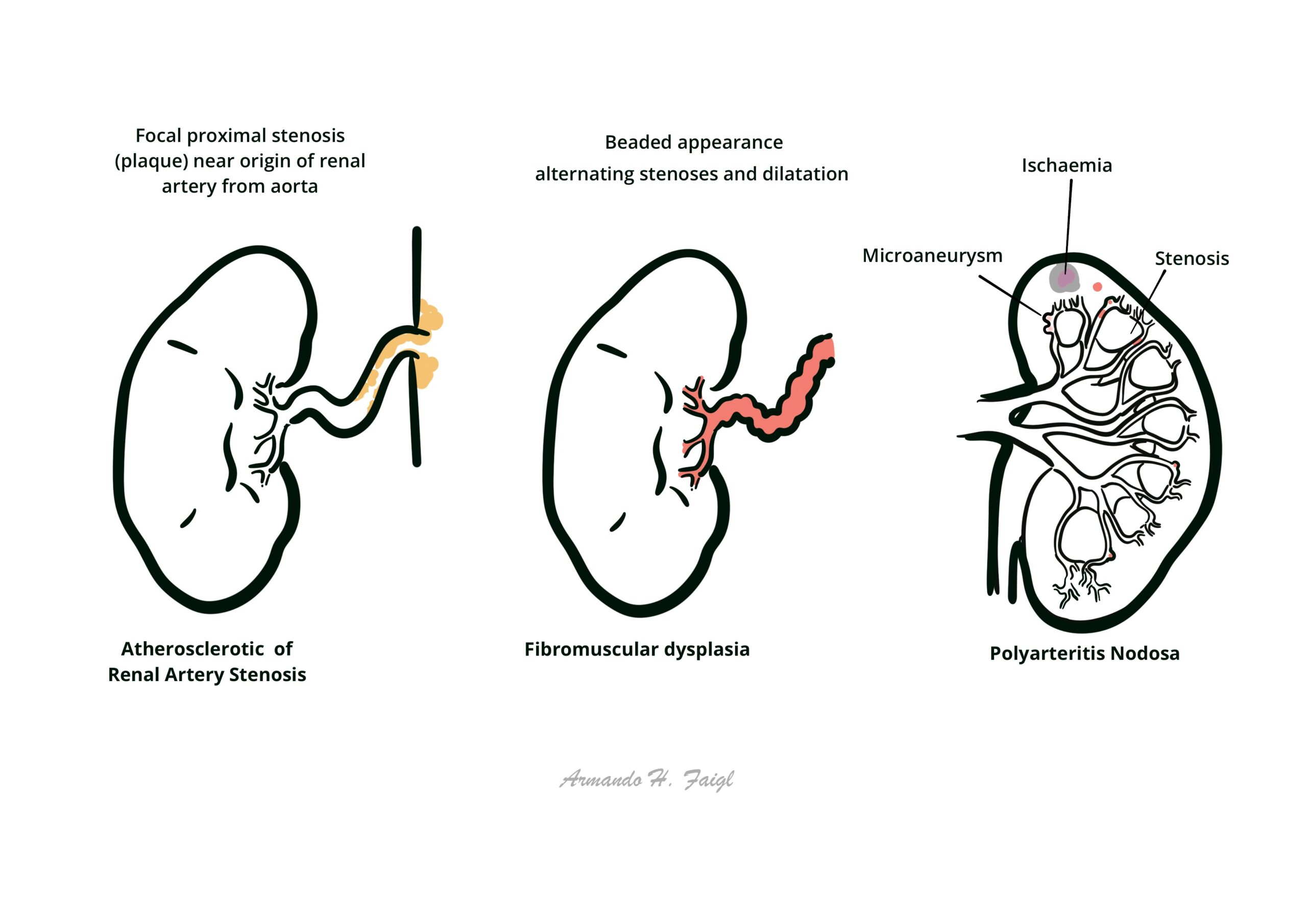
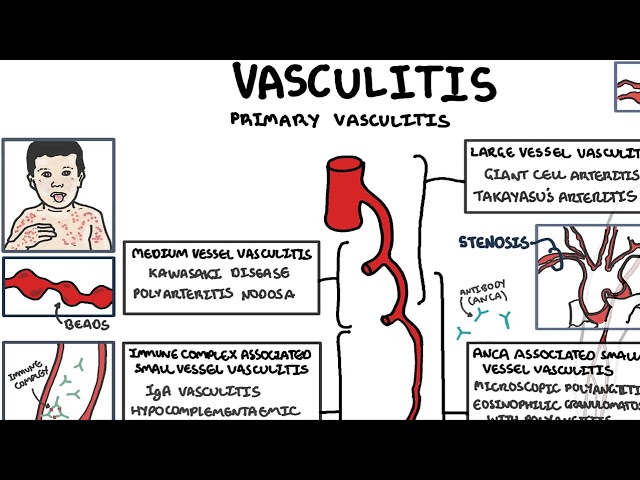
Polyarteritis Nodosa (PAN) is a necrotising vasculitis that affects medium-sized muscular arteries, leading to transmural inflammation, fibrinoid necrosis, and subsequent aneurysm formation or ischemia. It does not involve arterioles, capillaries, or venules, and is not associated with ANCA. PAN can affect any organ except the lungs. It typically presents in middle-aged adults, more commonly in men, and has been historically associated with hepatitis B infection.
Definition
Polyarteritis Nodosa (PAN): A systemic necrotising vasculitis involving medium-sized arteries, leading to organ ischemia and infarction.
Necrotising vasculitis: Inflammation of the vessel wall with fibrinoid necrosis and leukocytic infiltration.
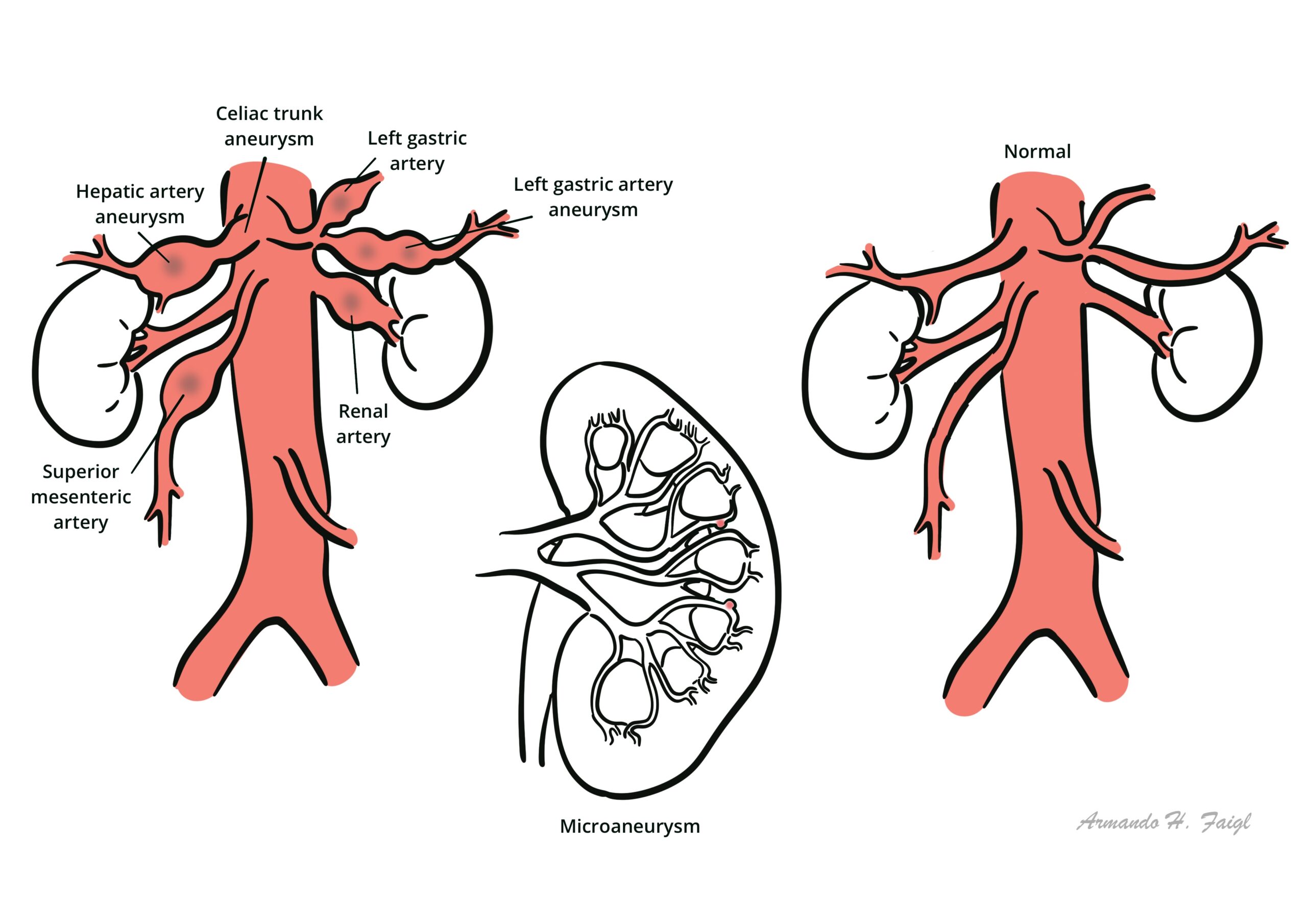
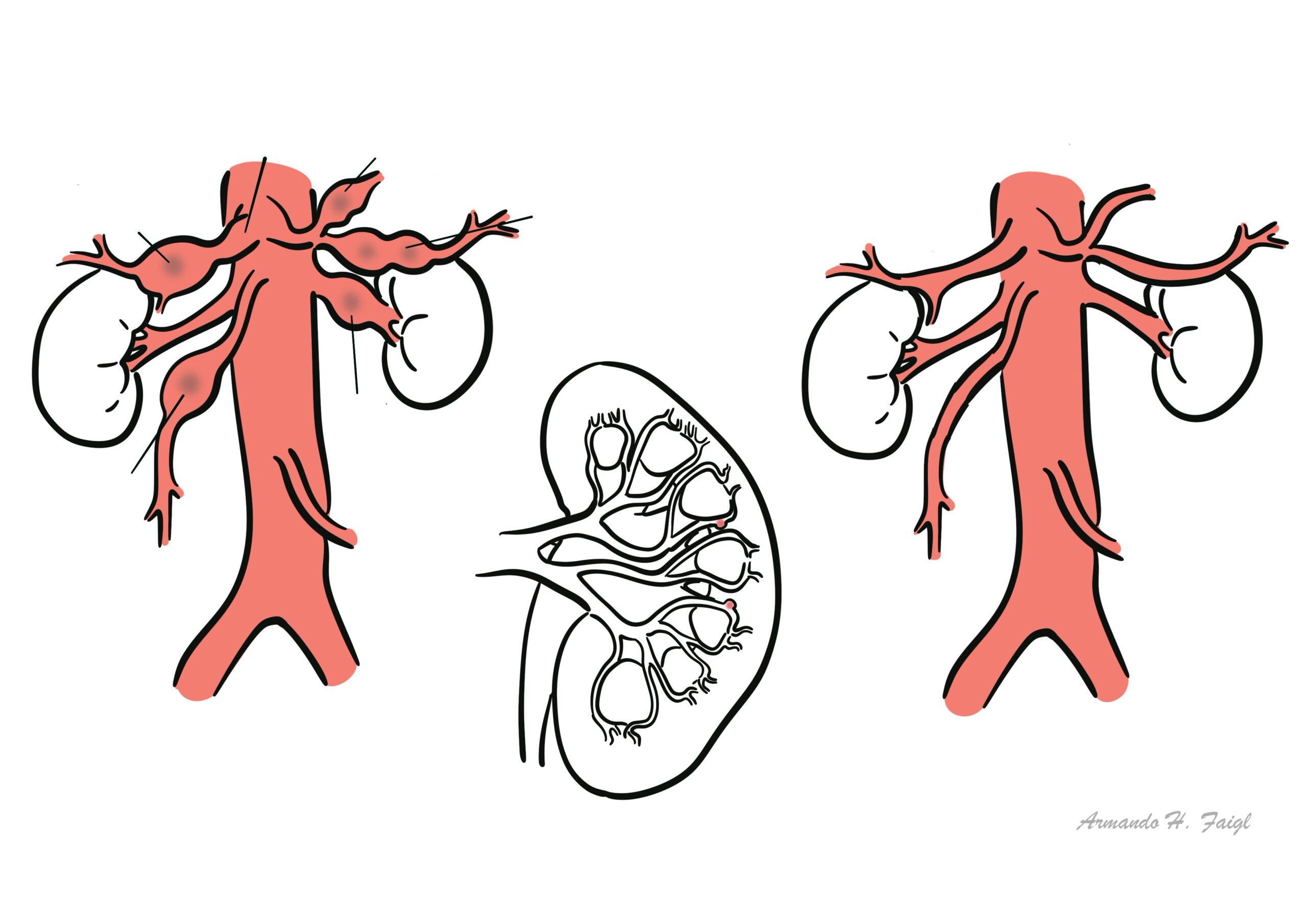
Microaneurysm: Localized arterial dilatation due to vessel wall weakening from inflammation.
Mononeuritis multiplex: Asymmetric sensorimotor peripheral neuropathy affecting multiple nerves due to vasculitis.
PAN = medium-sized arteries, ANCA-negative, lungs spared.
Anatomy & Physiology
- Medium-sized muscular arteries supply organs and major tissues; examples include renal, mesenteric, and hepatic arteries.
- In PAN, vasculitis leads to thrombosis, aneurysm, or rupture, causing tissue infarction or hemorrhage.
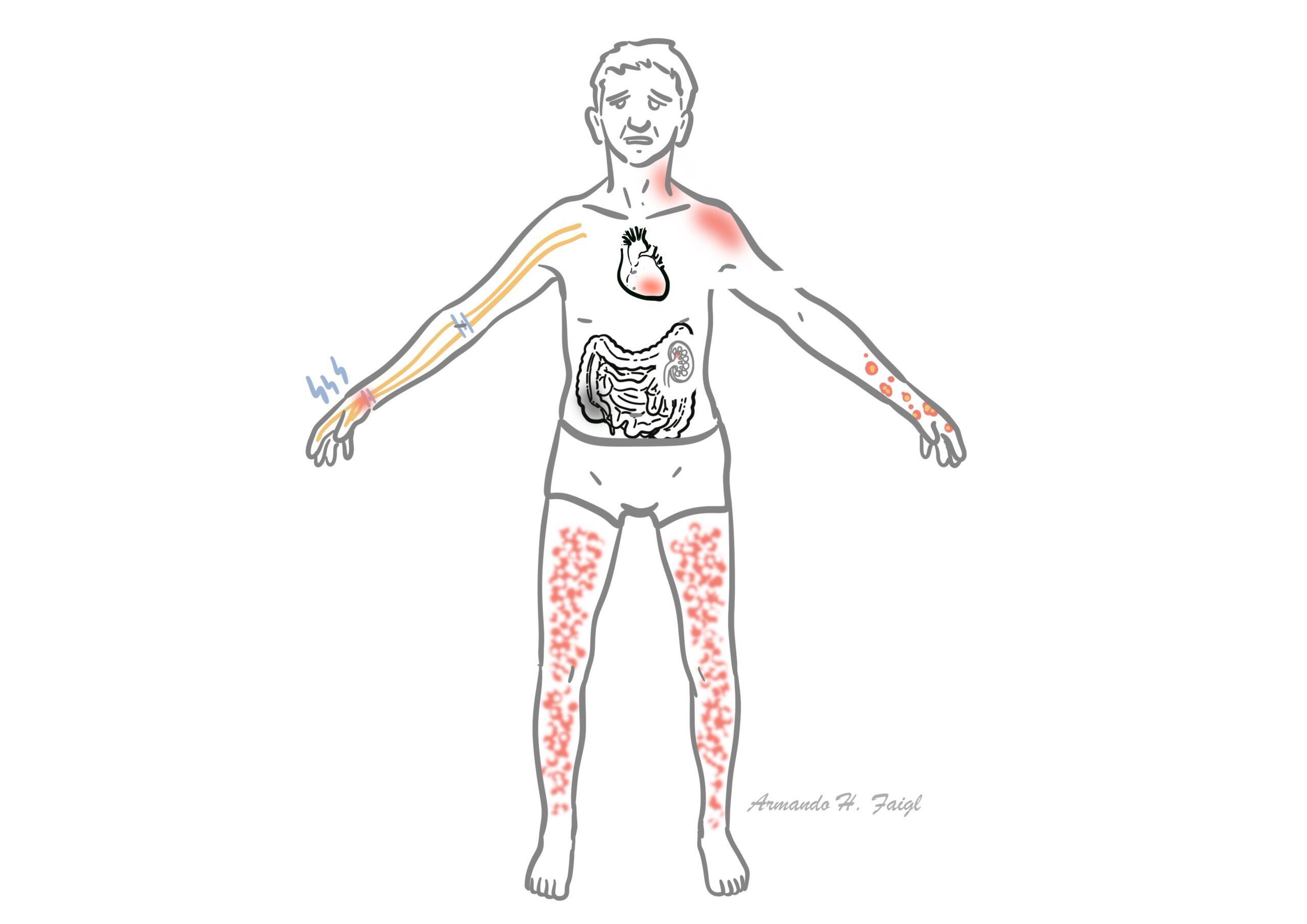
- Organs commonly affected: skin, nerves, kidneys, GI tract, heart, testes.
The lungs are typically spared, differentiating PAN from other vasculitides.
Aetiology & Risk Factors
Aetiology
- Idiopathic in most cases
- Hepatitis B virus (HBV) (strong historical association, <10% in modern cohorts)
- Rarely linked to hairy cell leukemia or drug reactions
- Male sex
- Age 40–60
- HBV or HCV infection
- Immunosuppressive states
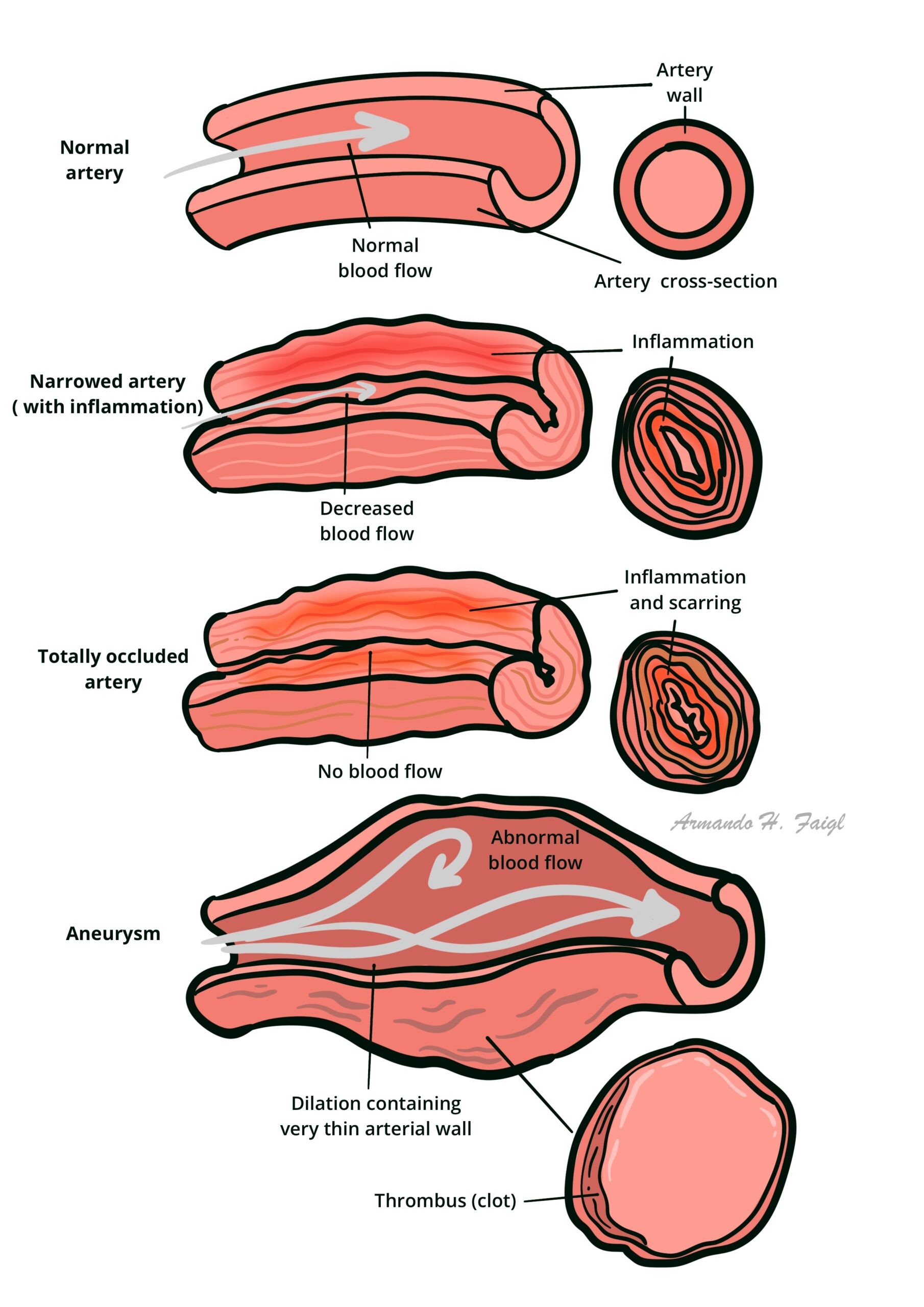
Pathophysiology
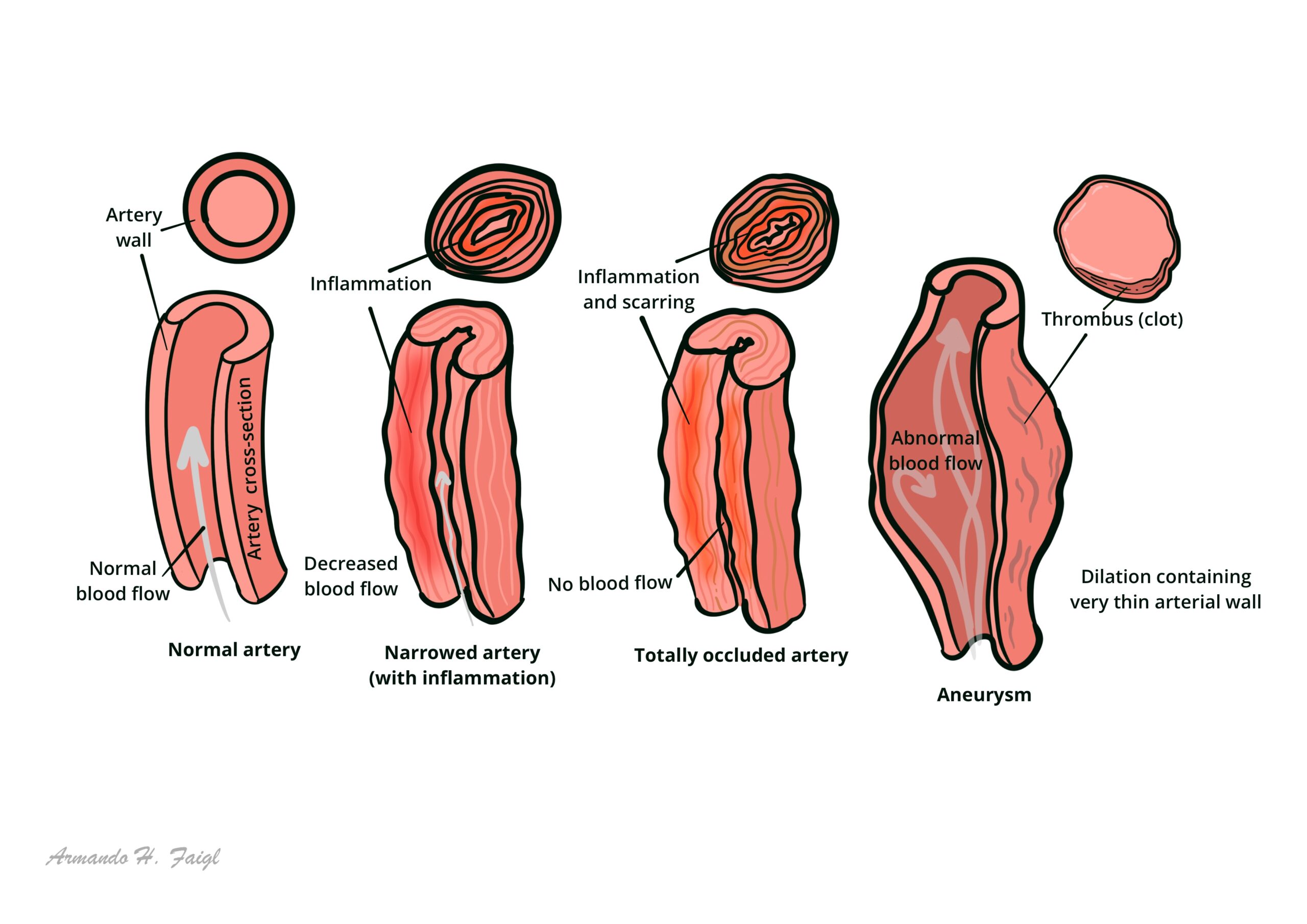
- Immune complex-mediated inflammation of medium-sized arteries
- Results in transmural necrotising inflammation, leukocyte infiltration
- Leads to fibrinoid necrosis, weakening of vessel wall → microaneurysms
- Aneurysms can rupture or thrombose → downstream organ ischemia or infarction
- Disease progression is segmental and skips regions (skip lesions)
Mesenteric or renal aneurysms on angiography = classic PAN feature.
Clinical Manifestations
| System | Manifestations |
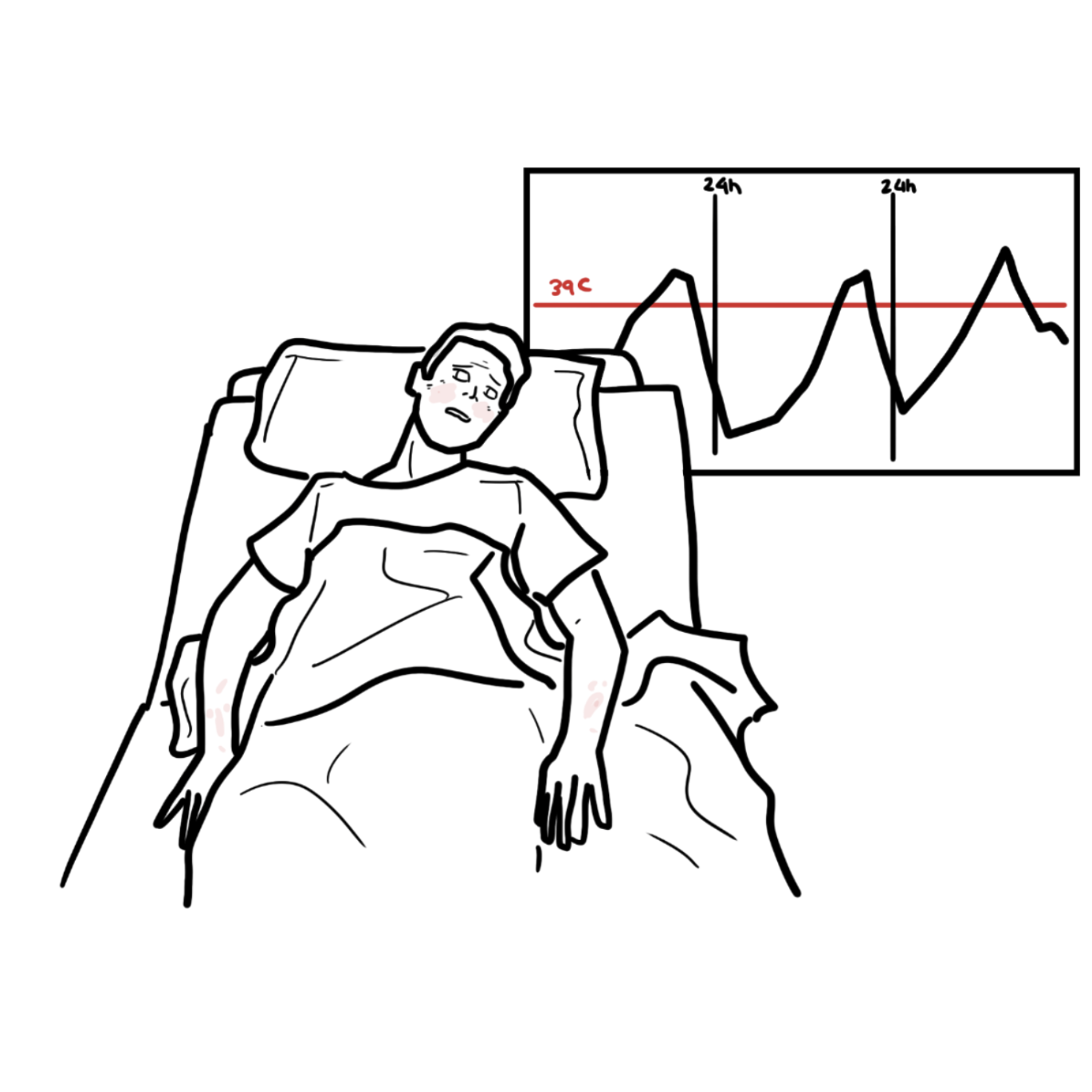
| Constitutional | • Fever, weight loss, malaise, fatigue |
| Skin | • Livedo reticularis • Palpable purpura • Nodules • Ulcers |
| Neurologic | • Mononeuritis multiplex • Peripheral neuropathy |
| Renal | • Renal infarcts • Hypertension (from renal ischemia) |
| GI | • Postprandial abdominal pain (intestinal angina) • GI bleeding • Bowel infarction or perforation |
| Cardiac | • Myocarditis, coronary vasculitis, arrhythmias |
| Musculoskeletal | • Myalgias • Arthralgias |
| Testicular | • Painful testicular tenderness (vasculitis) |

Triad Livedo reticularis, Mononeuritis multiplex, Renal/midline aneurysms on angiography.
Diagnosis
| Classification Criteria (ACR 1990) (≥3 of 10) |
| Weight loss >4 kg |
| Livedo reticularis |
| Testicular pain or tenderness |
| Myalgias or muscle weakness |
| Mononeuritis multiplex |
| Diastolic BP >90 mmHg |
| Elevated BUN or creatinine |
| Hepatitis B virus infection |
| Arteriographic abnormality (aneurysms, stenosis) |
| Biopsy showing necrotising vasculitis of medium-sized artery |
Investigations
- Bloods: ↑ ESR/CRP, anemia, leukocytosis
- Negative ANCA (distinguishes from MPA or GPA)
- HBV serology
- Angiography: microaneurysms in mesenteric/renal arteries
- Nerve or skin biopsy: necrotising inflammation of medium arteries
Differential Diagnoses
- Microscopic polyangiitis (ANCA+, glomerulonephritis)
- Takayasu arteritis
- GPA (ENT involvement, lung nodules, ANCA+)
- Fibromuscular dysplasia
- Infective endocarditis
- Cholesterol emboli syndrome
Classification
- Primary (idiopathic) PAN
- Secondary PAN – associated with HBV, HCV, malignancy
Treatment
| Severity | Treatment Strategy |
| Mild-moderate | • High-dose glucocorticoids alone |
| Severe (organ-threatening) | • Glucocorticoids + cyclophosphamide |
| HBV-associated | • Antivirals + short-course steroids + plasmapheresis |
| Refractory/relapse | • Consider rituximab, azathioprine, or methotrexate as maintenance |
Always screen for HBV, HCV, HIV, TB before starting immunosuppressants.
Complications & Prognosis
- Renal failure
- Bowel infarction/perforation
- Stroke
- Myocardial infarction
- Testicular infarction
- Peripheral neuropathy
Poor Prognostic Factors (Five-Factor Score)
- Proteinuria >1 g/day
- Renal insufficiency
- GI involvement
- CNS involvement
- Cardiomyopathy
- Age >65
References
- Pagnoux C. Polyarteritis nodosa and microscopic polyangiitis. Best Pract Res Clin Rheumatol. 2005;19(2):263–276.
- Guillevin L, et al. The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides. Arthritis Rheum. 2011;63(5):1251–1259.
- Jennette JC, et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1–11.
- de Boysson H, et al. Polyarteritis nodosa: diagnosis and management. Curr Opin Rheumatol. 2020;32(1):30–36.
- Mahr A, et al. Epidemiology of polyarteritis nodosa. Clin Exp Rheumatol. 2006;24(2 Suppl 41):S3–S7.








Members only discussions coming soon…