

Henoch–Schönlein Purpura (IgA Vasculitis)

Overview
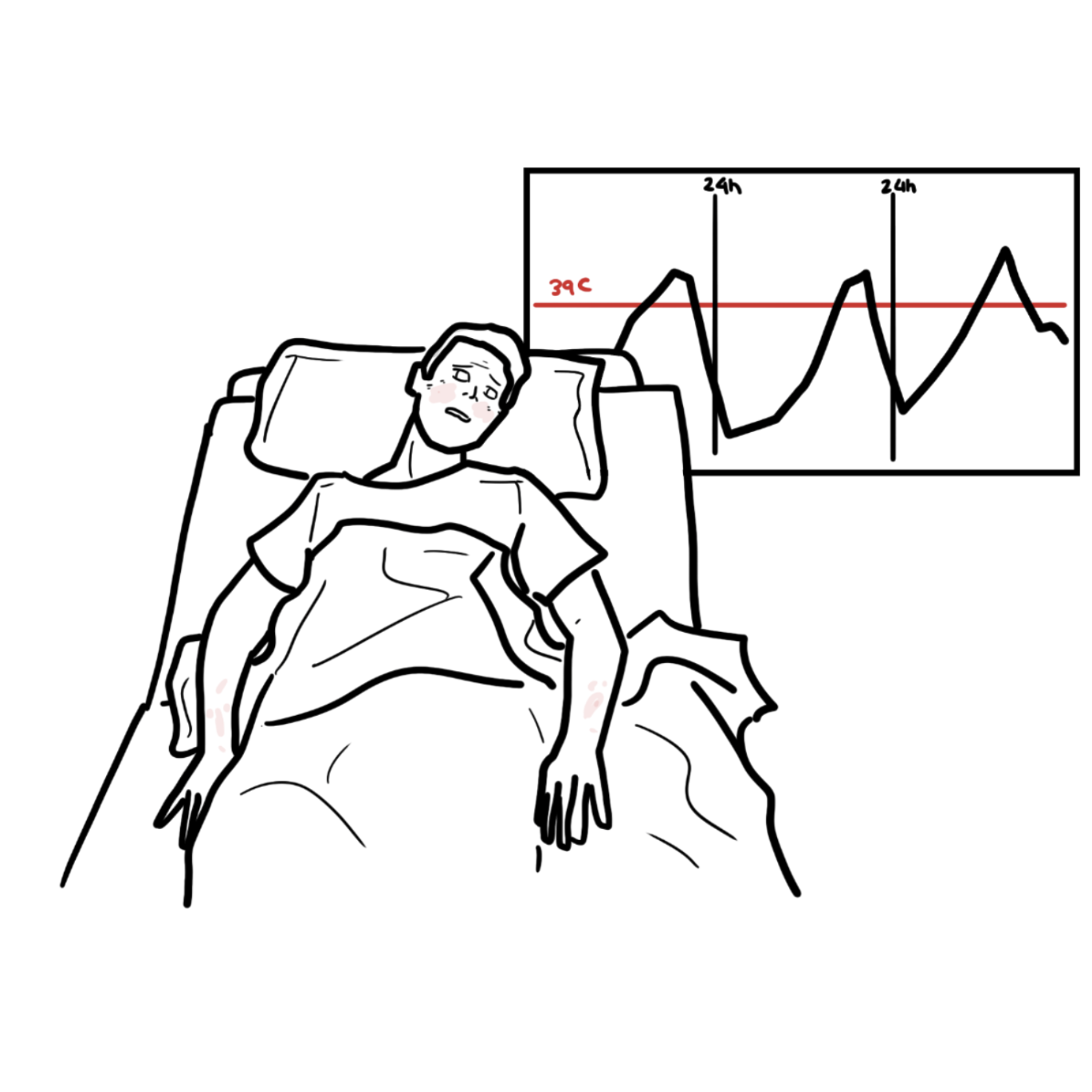
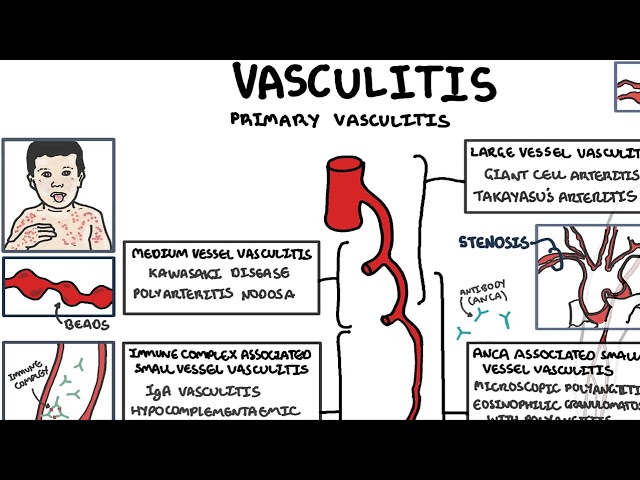
Henoch–Schönlein purpura (HSP), now termed IgA vasculitis, is the most common systemic vasculitis in children, characterised by IgA1-dominant immune complex deposition in small vessels, particularly affecting the skin, joints, gastrointestinal tract, and kidneys. It predominantly occurs in children aged 3–10 years, with a slight male predominance, and often follows an upper respiratory tract infection. The incidence is approximately 10–30 per 100,000 children per year. The disease is usually self-limiting but can have significant morbidity when renal involvement occurs.
Definition
IgA vasculitis: Small-vessel vasculitis with IgA-dominant immune complex deposition.
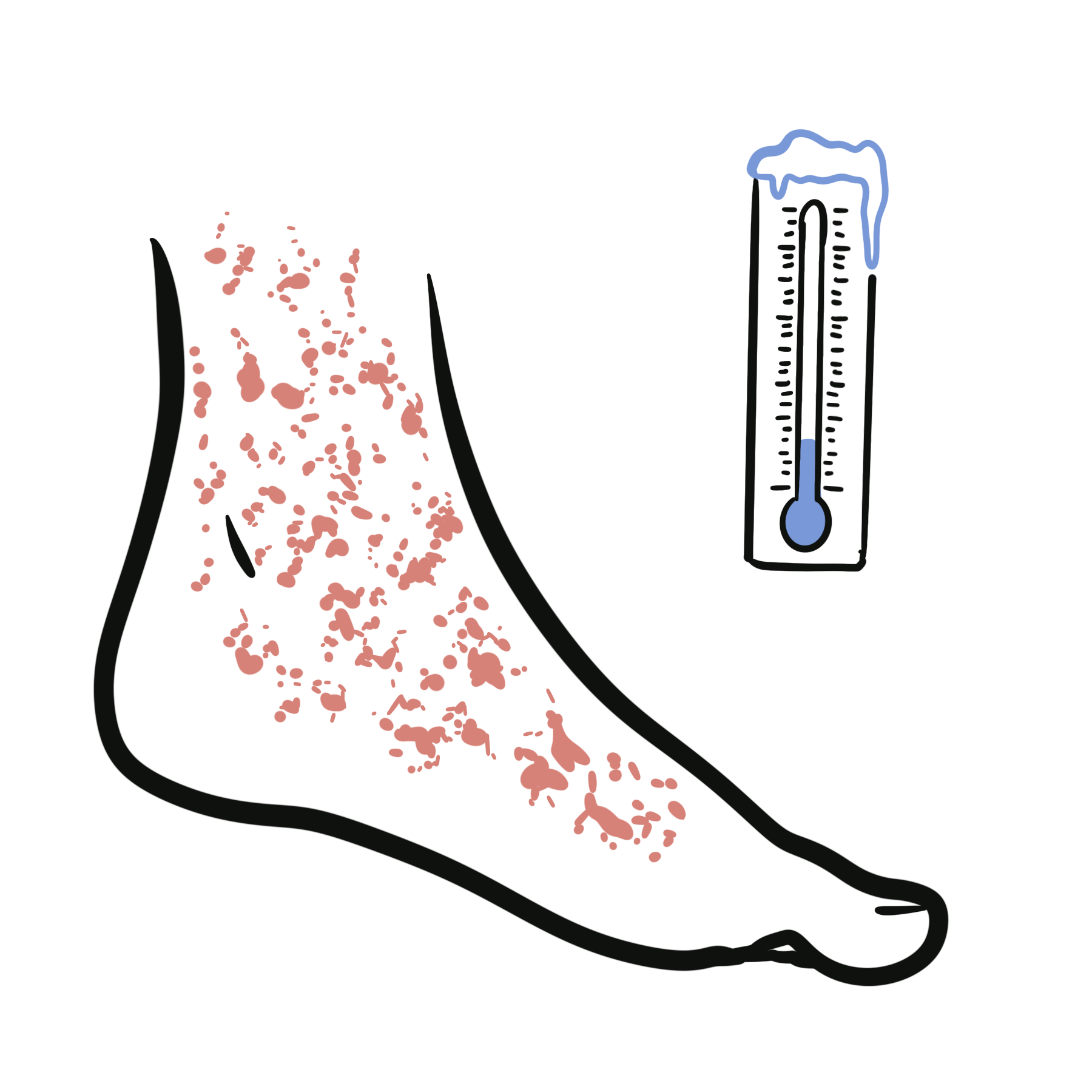
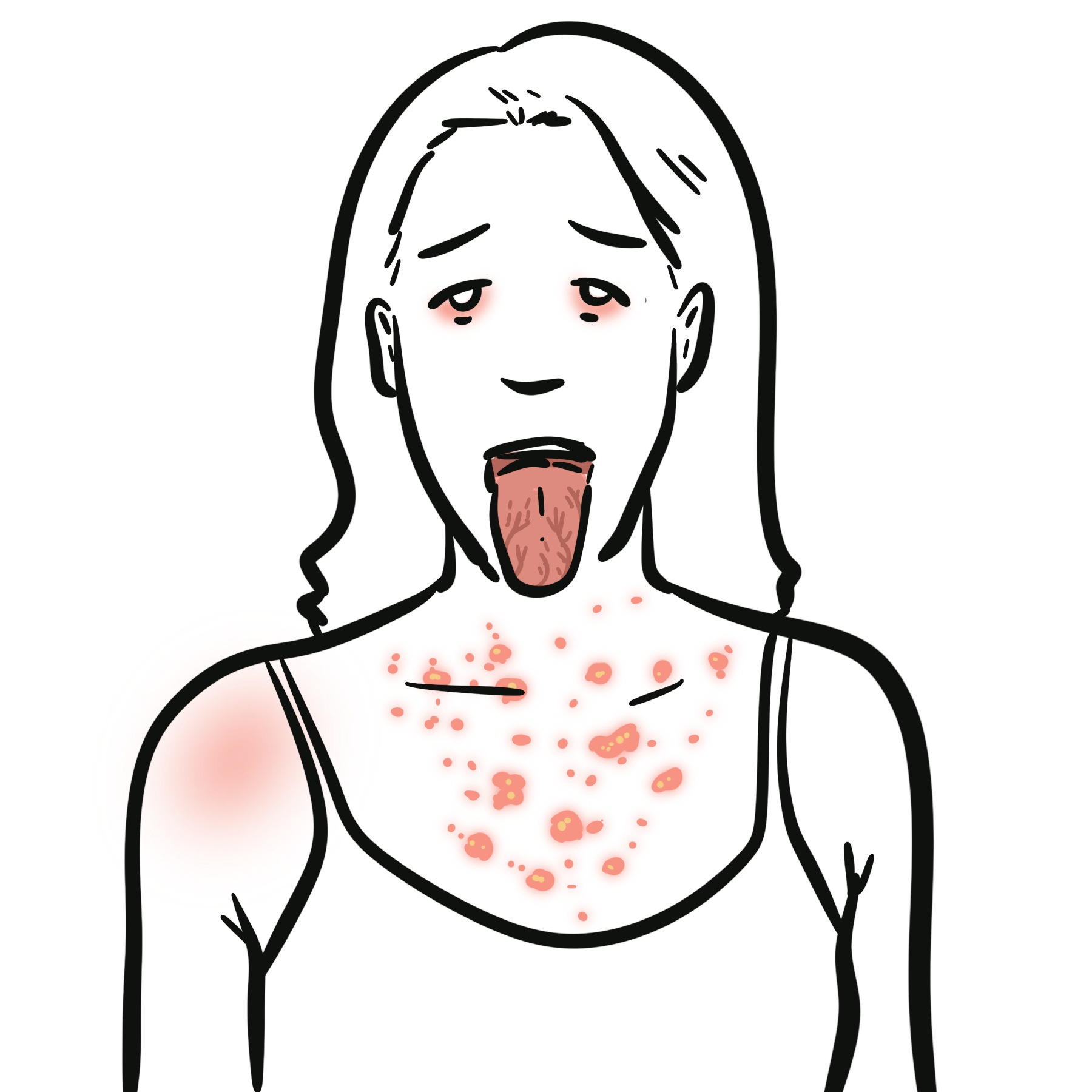
Palpable purpura: Non-blanching, raised skin lesions due to vascular inflammation.
IgA nephritis (IgAVN): Renal involvement characterised by IgA deposition in glomeruli.
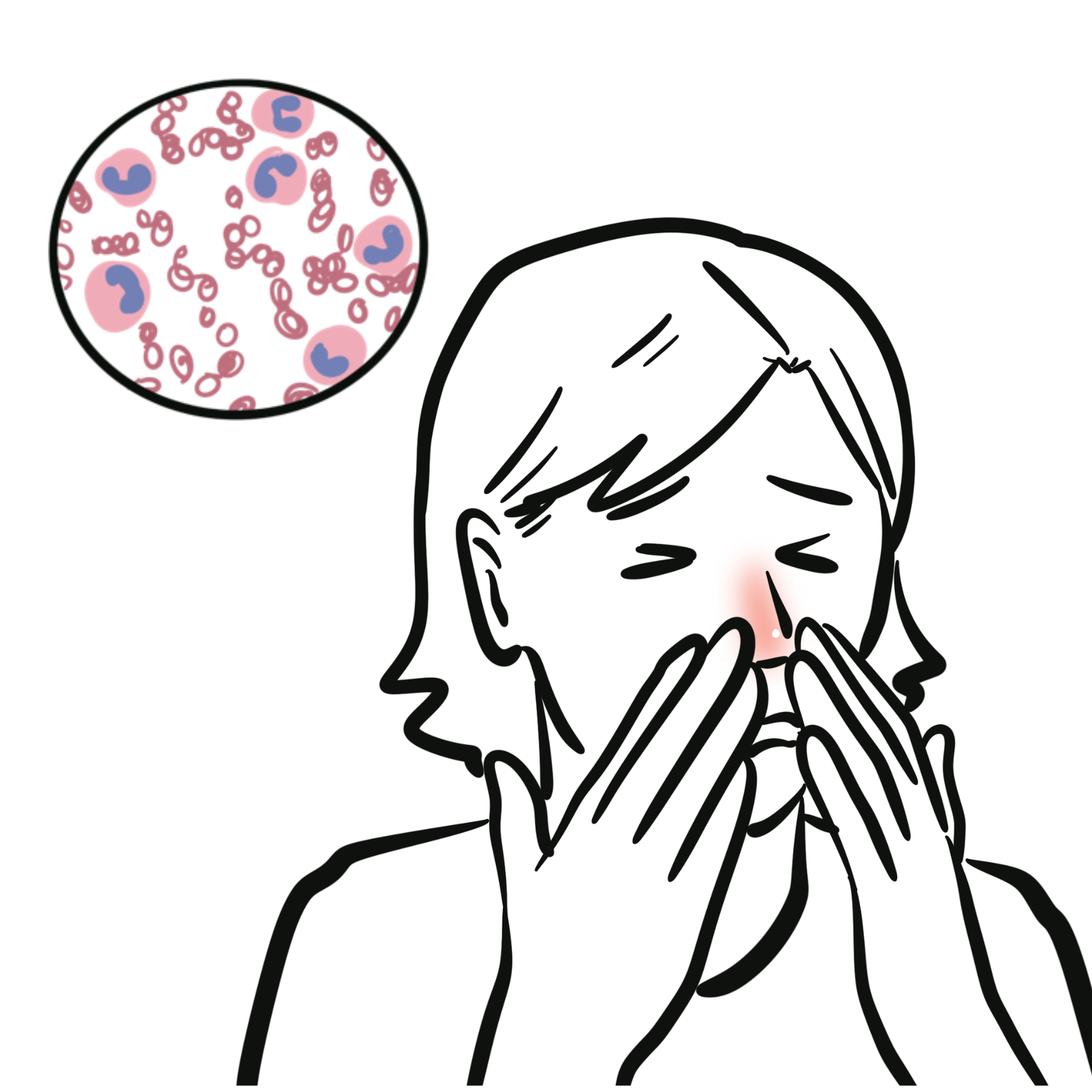
Leukocytoclastic vasculitis: Neutrophil-mediated small-vessel inflammation.
HSP = IgA-mediated small vessel vasculitis in children.
Anatomy & Physiology
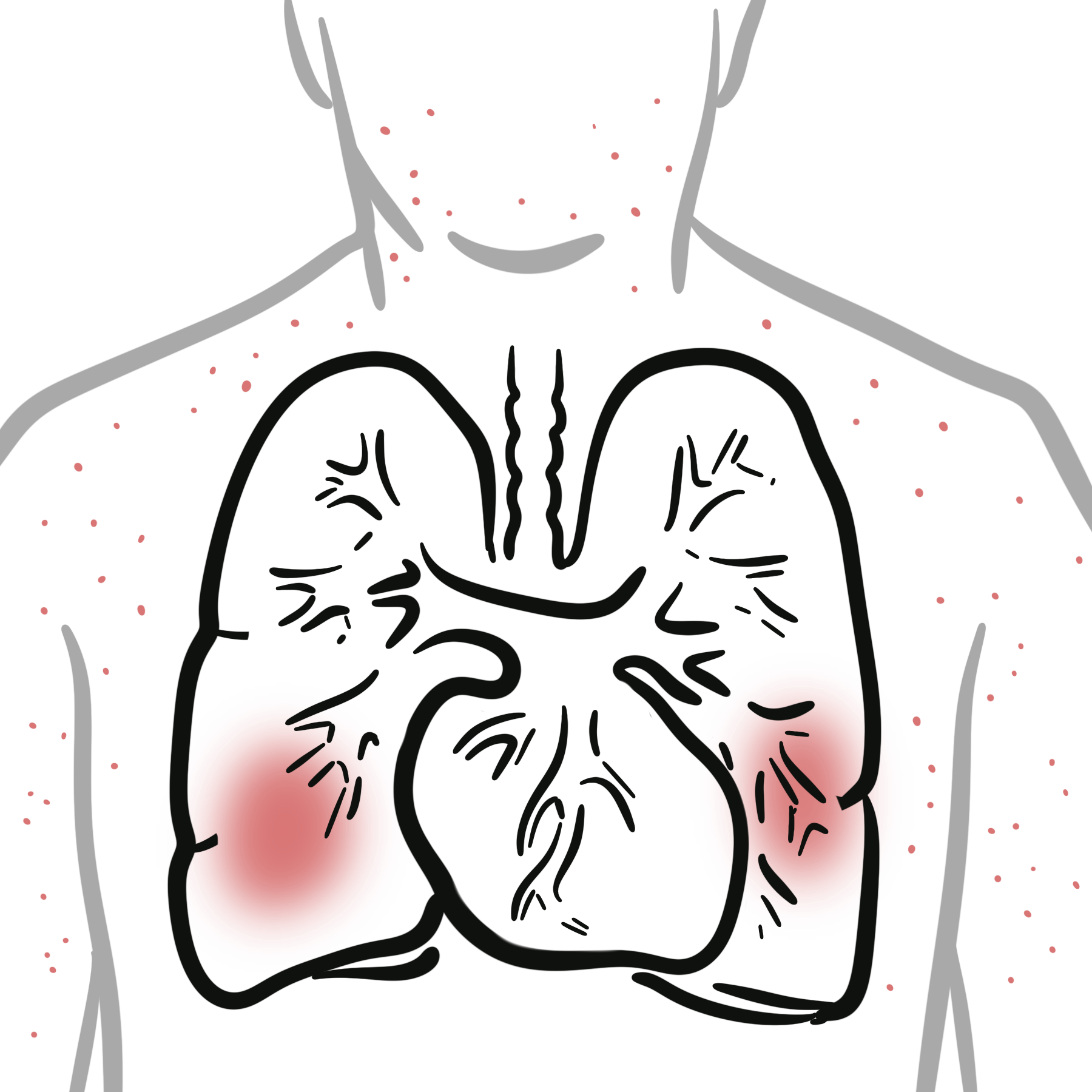
- Small vessels: Capillaries, venules, arterioles—sites of immune complex deposition
- IgA function: Mucosal immunity; produced in response to infections
- Complement system: Alternative and lectin pathways activated by immune complexes
Aetiology & Risk Factors
Aetiology
- Post-infectious immune response (most commonly URTI)
- Viral or bacterial triggers
- Immune dysregulation with IgA overproduction
- Age 3–10 years
- Male sex
- Recent infection
- Seasonal variation (winter/spring)
Pathophysiology
- Trigger (infection) → increased IgA production
- Formation of IgA immune complexes
- Deposition in small vessels
- Complement activation → inflammation
- Vascular damage → purpura, organ involvement
Immune complex disease → multi-organ involvement.
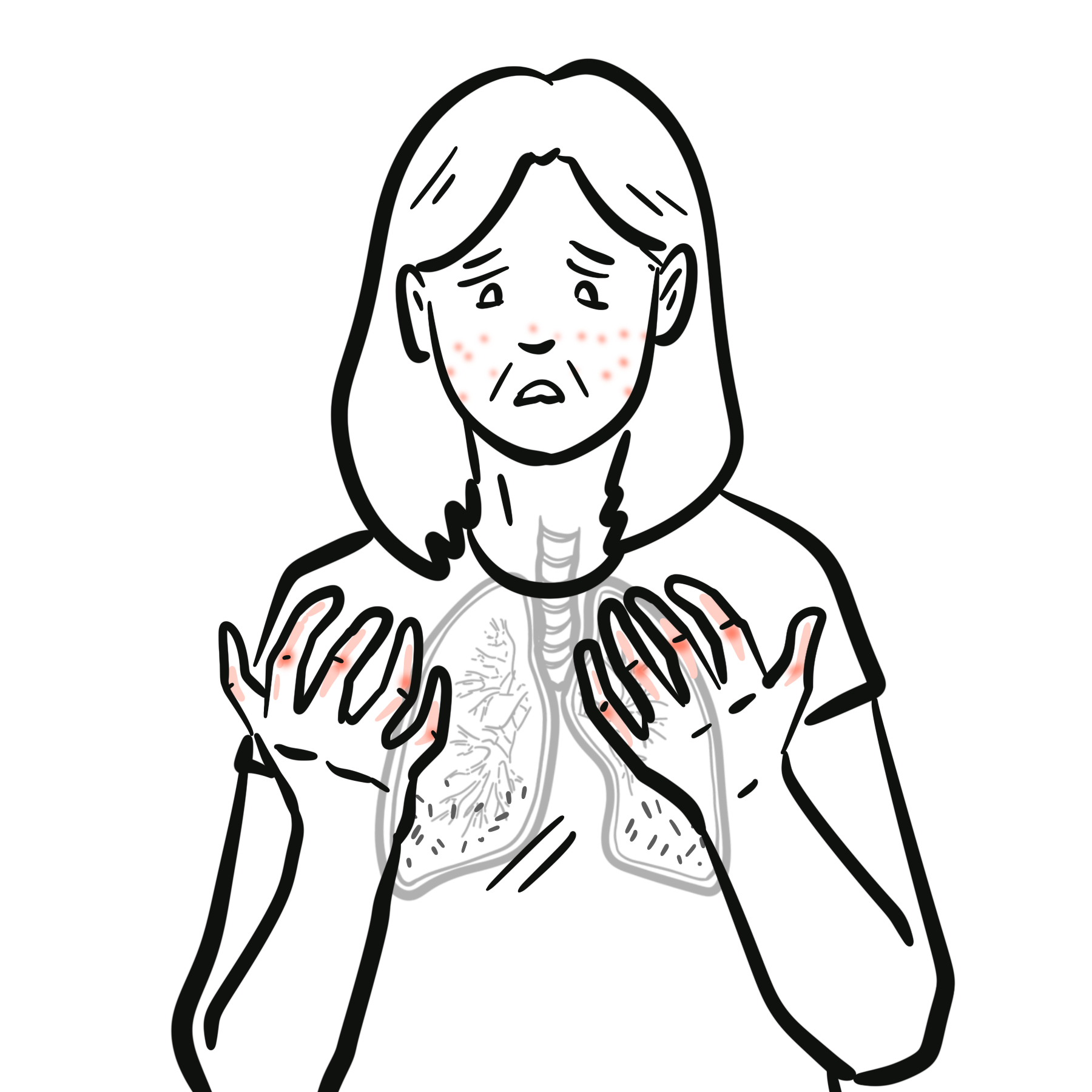
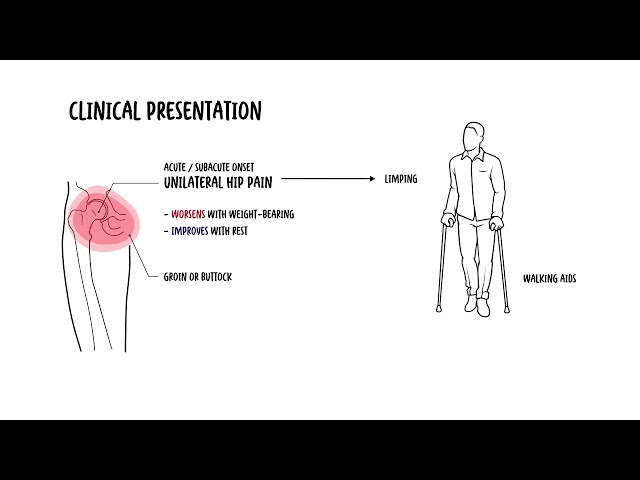
Clinical Manifestations
- Palpable purpura (legs, buttocks)
- Arthralgia/arthritis
- Abdominal pain (colicky)
- GI bleeding
- Haematuria ± proteinuria
- Oedema (hands, feet, scrotum)
Classic tetrad Purpura, Arthralgia, Abdominal pain, Renal involvement.
Diagnosis
EULAR/PRINTO/PRES Criteria (2008 validated):
- Mandatory: Purpura/petechiae
- Plus ≥1:
- Abdominal pain
- Arthritis/arthralgia
- Renal involvement
- IgA deposition on biopsy
- Urinalysis (haematuria, proteinuria)
- Bloods: CRP, ESR, renal function
- Skin biopsy (IgA deposition) if uncertain
- Imaging (USS abdomen if intussusception suspected)
Differentials
Diagnosis is mainly clinical.
Treatment
- Mild pain
- Paracetamol
- NSAIDs (if not older)
- Elevate oedematous lower limb
- Moderate-severe pain
- Admit
- IV steroids OR oral steroids
- Paediatric consult
- Elevate oedematous lower limb
Ongoing management
- Regular GP/Paediatrician review for progress and complications
Complications & Prognosis
- Intussusception
- GI bleeding
- Renal disease → CKD
- Recurrence
- Usually self-limiting in children
- Renal involvement determines outcome
- Poor prognostic factors:
- Persistent proteinuria
- Hypertension
- Older age
References
- Ozen S, et al. EULAR/PRINTO/PRES criteria for IgA vasculitis. Ann Rheum Dis. 2010.
- Weiss PF. IgA vasculitis. Lancet. 2015.
- KDIGO Guidelines. Glomerular diseases. 2021.







Members only discussions coming soon…