

Adult onset Still's Disease
Overview
Adult Onset Still’s Disease (AOSD) is a complex multisystemic autoinflammatory disease characterised by recurrent episodes of spiking fever (> 39–40°C), pink–salmon transient skin rash, and the presence of arthralgia or polyarthritis. First described by Eric Bywaters in 1971 it closely resembles systemic onset juvenile idiopathic arthritis (Still’s disease).
- retrospective observational study in Japan found an incidence of 0.22 and 0.34 cases per 100,000 and a prevalence of 0.73 and 1.47 cases per 100,000 for males and females, respectively
- bimodal age distribution, with one peak between the ages of 15 and 25 and the second between the ages of 36 and 46.
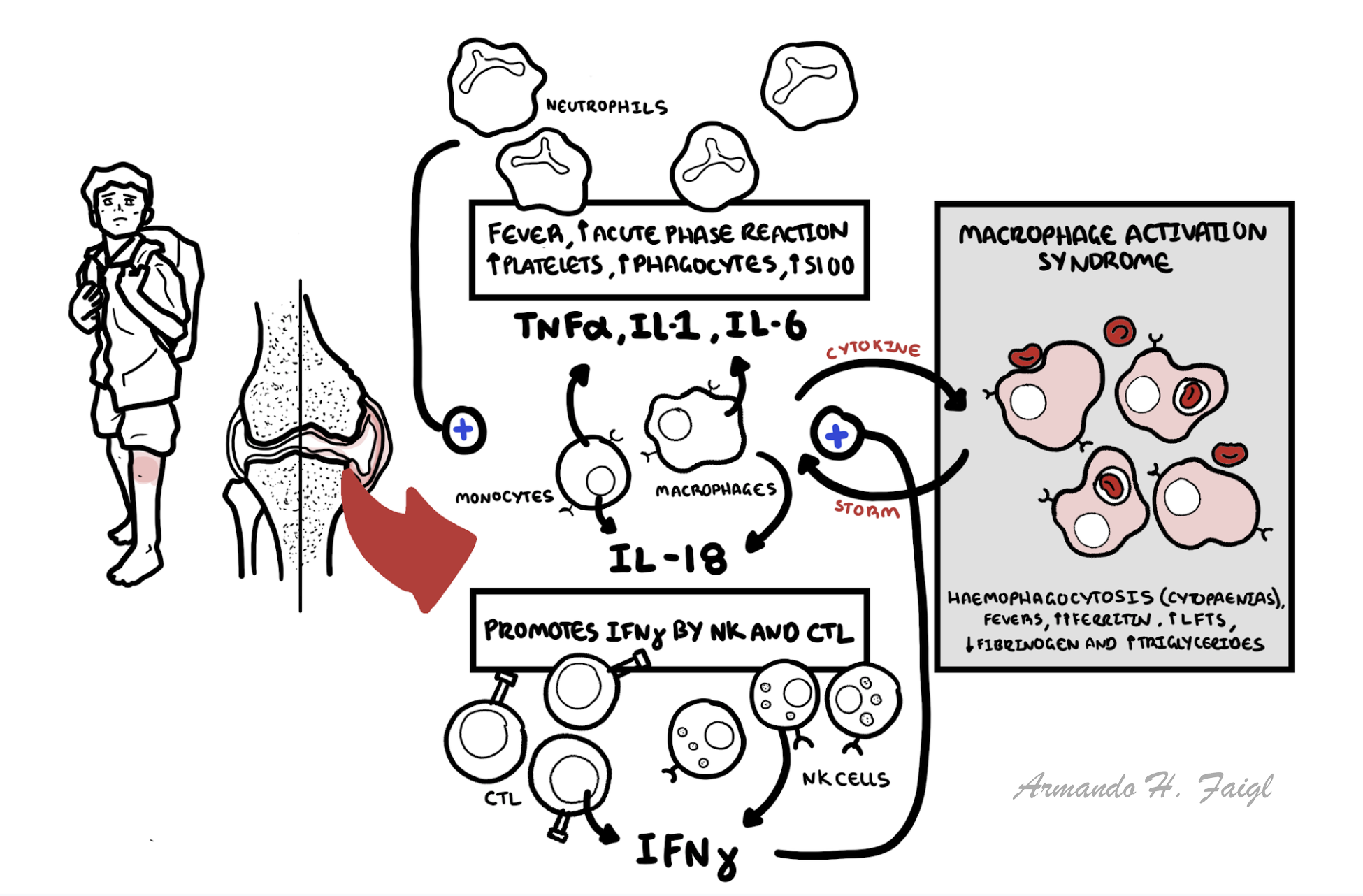
Pathophysiology
AOSD is a polygenic and systemic autoinflammatory disease. Pathophysiology is thought to be intense activation of innate immune system and overproduction of several proinflammatory cytokines. Including IL1, Il6 TNFa and IL18.
Clinical Manifestations
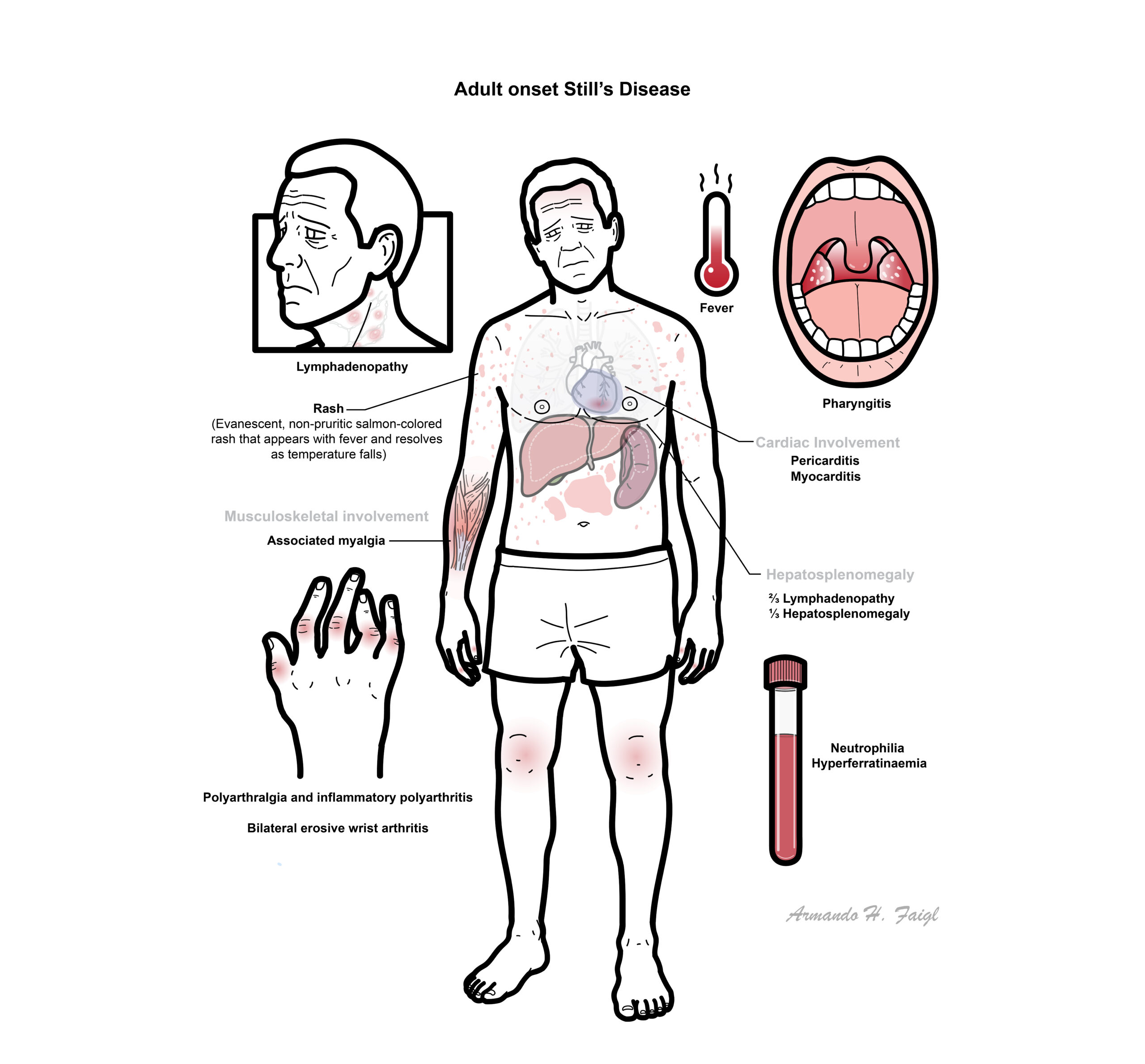
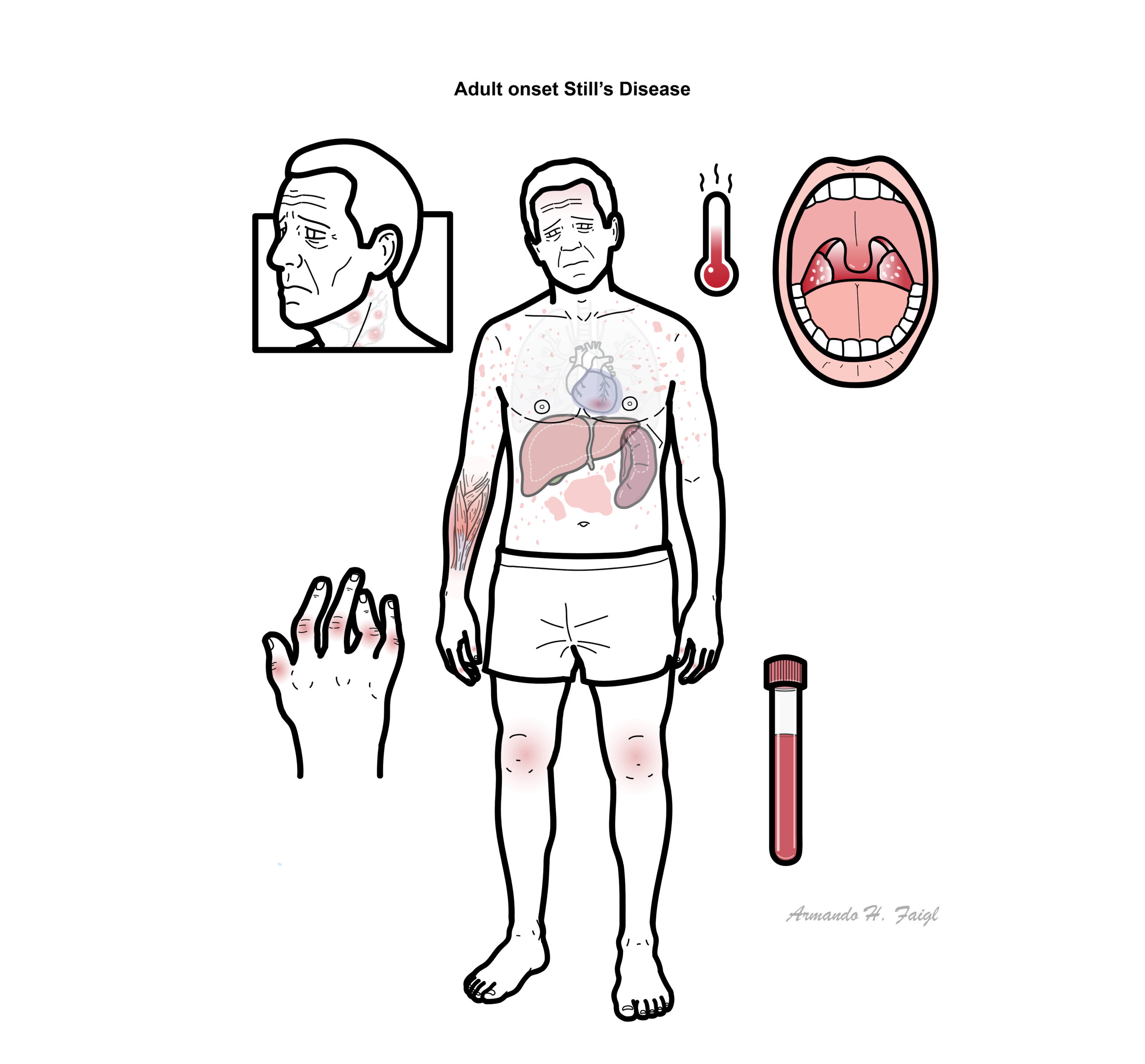
AOSD include fever, rash, and arthritis or arthralgia; each occur in about 75 to 95 percent of patients. Patients typically present after weeks to months of symptoms.
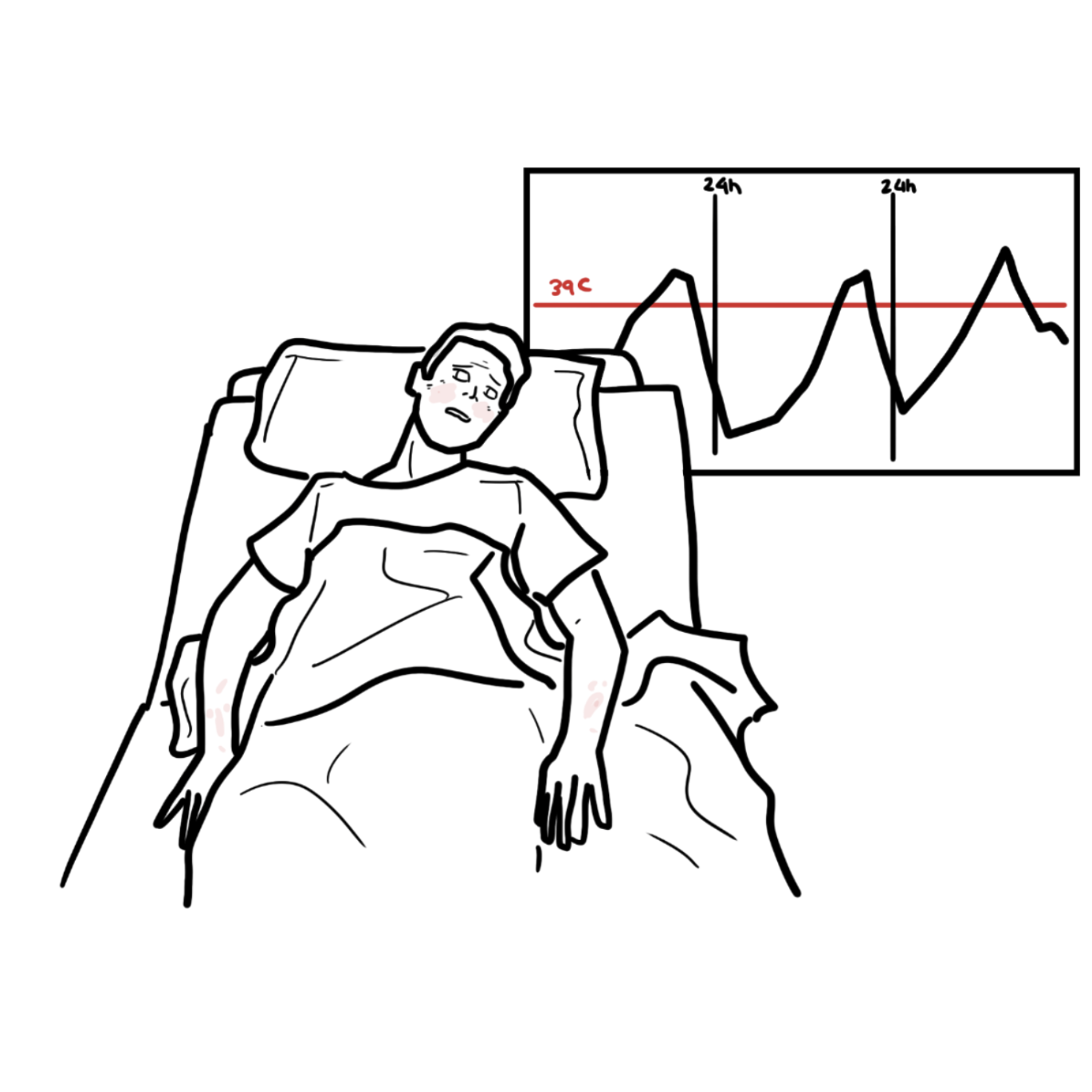
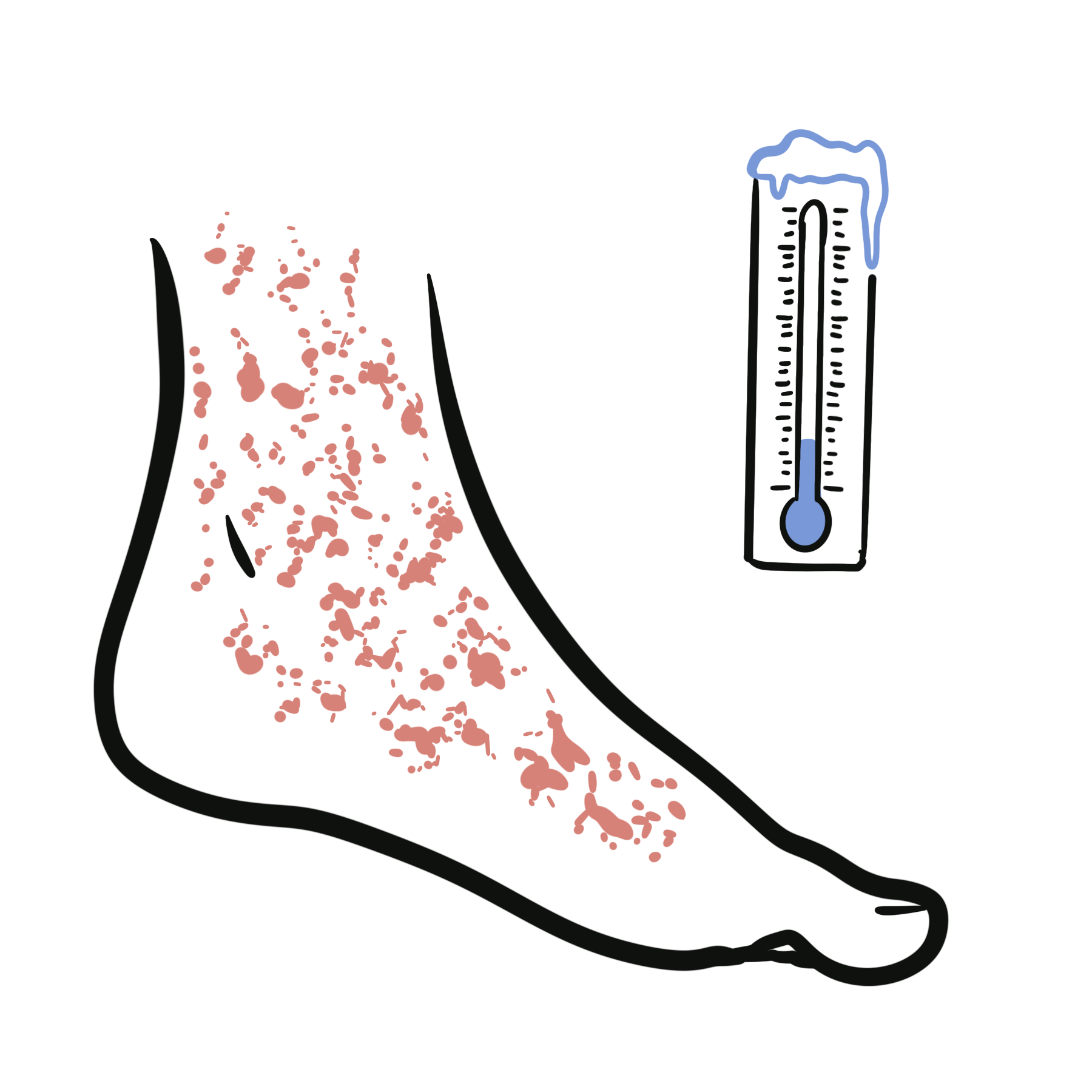
Fever
- The fever curve is the most important diagnostic criterion for AOSD
- Typically a Quotidian pattern fever (a daily recurring fever ≥39°C)
- Double-quotidian (two fever spikes per day) can occur
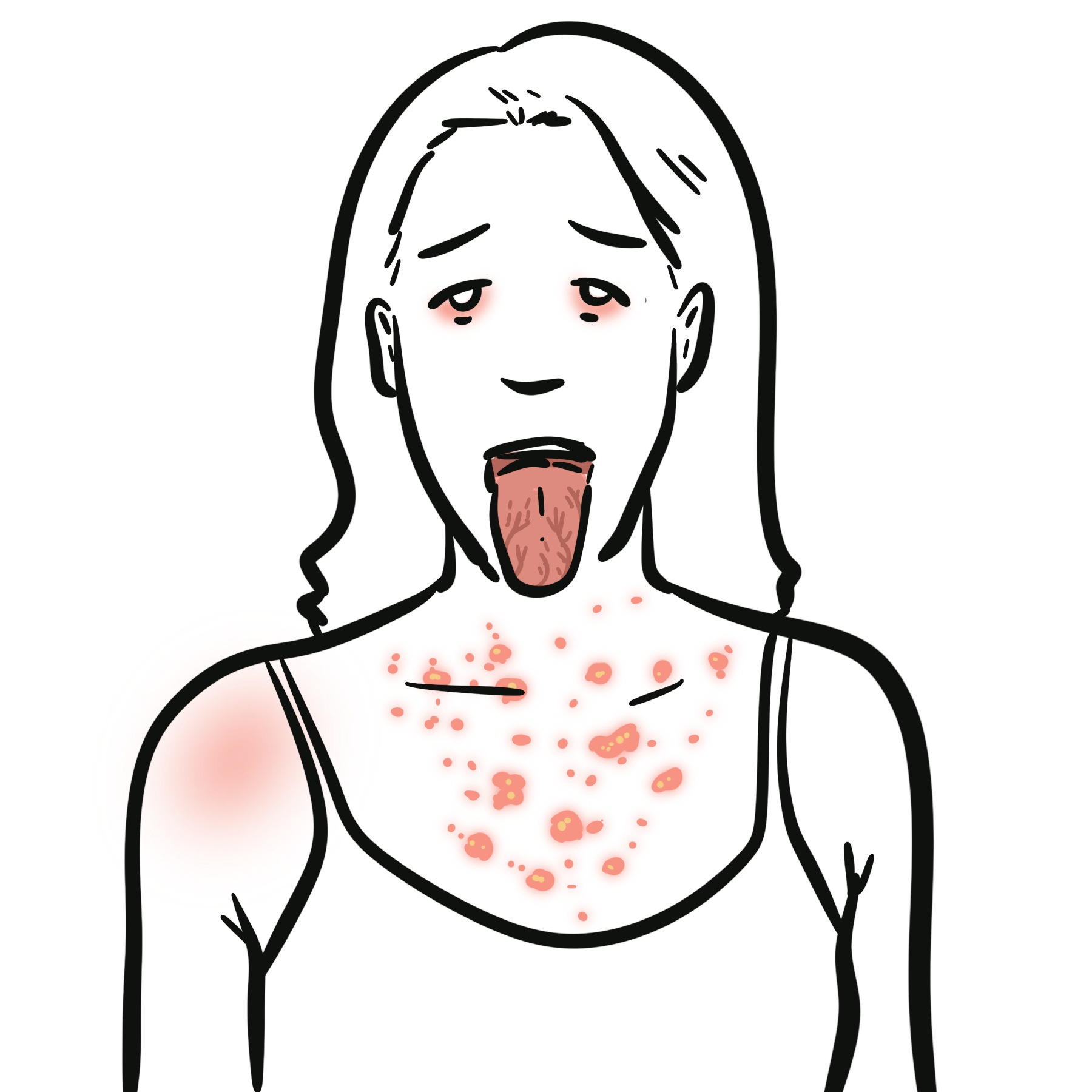
Rash
- Evanescent, salmon colour, non pruritic skin rash
- Erupts during fevers and subsides with it.
- Urticarial lesions can occur
Musculoskeletal involvement
- Polyarthralgia (common)
- Polyarthritis
- Myalgia
Pharyngitis — A severe, nonsuppurative pharyngitis is common
Hepatosplenomegaly with associated lymphadenopathy
- ⅔ lymphadenopathy
- ⅓ hepatosplenomegaly
Cardiac involvement
Classification
| Yamaguchi Criteria | ||
| Major Criteria | Minor Criteria | Exclusion Criteria |
| Fever ≥39°C>°C lasting ≥7 days | Sore throat | Infections |
| Arthralgias or arthritis for ≥14 days | Hepatomegaly or splenomegaly | Other rheumatic disease |
| Typical rash | Lymphadenopathy | Malignancies |
| Pharyngitis | Abnormal aminotransferases | |
| WBC count >10 with Neutrophils ≥80% | Negative rheumatoid factor and ANA | |
Criteria: Five or more criteria are required. Two or more criteria must be major. Typical rash is an evanescent, salmon-coloured rash that erupts during fevers and subsides with it.
| Fautrel’s Criteria | |
| Major Criteria | Minor Criteria |
| Spiking fever ≥39°C | Maculopapular rash |
| Arthralgias | Leukocytosis ≥10,000/µL |
| Transient erythema | |
| Pharyngitis | |
| Neutrophils ≥80% | |
| Glycosylated ferritin ≤20% | |
Criteria: Four or more major criteria are required, or three major and two minor criteria are required.
Investigations
- Liver derangement (ALT and AST marker of disease activity)
- Elevated WCC (>80% neutrophils)
- Elevated acute phase reactants
- Ferritin, fibrinogen
- Platelets
- ESR and CRP
- Blood cultures and polymerase chain reaction (PCR) tests
- Bone marrow biopsy to rule out haematological malignancy
- Lymph node biopsy to rule out haematological malignancy
- PET/CT scan to ule out malignancy and vasculitis
glycosylated fraction of ≤20 percent
Complications & Prognosis
- Erosive arthritis – Erosive bilateral wrist (ankylosis with wrist fusion) without structural damage to the MCPJ
- Fulminant hepatitis
- Disseminated intravascular coagulation or thrombotic thrombocytopenic purpura.
- Diffuse alveolar haemorrhage, pulmonary arterial hypertension, interstitial lung disease, and alveolar proteinosis
- Macrophage activation syndrome
Macrophage activation syndrome is a subtype of hemophagocytic lymphohistiocytosis (HLH). It occurs in the setting of systemic rheumatic disease, most commonly AOSD or JOSD. In AOSD up to 15% are affected. MAS and HLH are driven by a hyperinflammatory state or “cytokine storm”. Characterised by fever, hepatosplenomegaly, and multiple laboratory abnormalities including high levels of inflammation, high ferritin, cytopenias, and transaminitis. MAS is the leading cause of death for patients with AOSD. Prompt treatment involves glucocorticoids, IL1 inhibitor or IL6 inhibitor.
Typically three courses of the disease
- ⅓ Monocyclic course – without relapses.
- ⅓ polycyclic course – unpredictable periods of exacerbation
- ⅓ Chronic progressive course, which is the most frequent one, which is characterised by steady progression, continuous inflammation and often erosive joint involvement
Treatment
- Mild – NSAID/Colchicine/Corticosteroids
- Moderate/severe
- addition of DMARD: Azathioprine, Methotrexate or leflunomide
- Addition of bDMARD: Il1 inhibitor or IL6 inhibitor
- Refractory disease
- Cyclosporine
- Rituximab
- JAKi
References
- Bhargava J, Aggarwal A. Still Disease. StatPearls. Updated 2024. NCBI Bookshelf. Covers classic clinical features, ferritin, and Yamaguchi criteria. (NCBI)
- Fautrel B, Cimaz R, Lehmberg K, et al. EULAR/PReS recommendations for the diagnosis and management of Still’s disease in adults and children. Annals of the Rheumatic Diseases. 2024. Provides modern diagnostic and management guidance across Still’s disease. (EULAR)
- Leavis HL, Gerfaud-Valentin M, Jamilloux Y, et al. Management of adult-onset Still’s disease: evidence- and consensus-based recommendations by experts. Rheumatology. 2024. Useful for treatment approach, including IL-1 and IL-6 targeted therapy. (OUP Academic)
- Bindoli S, Doria A, Galozzi P. Adult-Onset Still’s Disease (AOSD): Advances in Clinical Features, Pathogenesis, and Treatment. Drugs. 2024. Good review for phenotype recognition, biomarkers, and treatment concepts. (PMC)
- Bindoli S, et al. Efficacy and safety of therapies for Still’s disease and macrophage activation syndrome: a systematic literature review informing the EULAR/PReS recommendations. Annals of the Rheumatic Diseases. 2024. Supports the role of IL-1 and IL-6 inhibition and treatment evidence. (Annals of the Rheumatic Diseases)
- Regmi A, et al. Macrophage Activation Syndrome in Adult-Onset Still’s Disease. 2025. Review of MAS as a severe complication, including ferritin and organ dysfunction clues. (PMC)
- Orphanet. Diagnostic criteria for adult onset Still’s disease (AOSD). Summary of Yamaguchi criteria requirements. (Orpha.net)
- Cai Z, et al. New advances in Still’s disease from children to adults: a review. 2024. Broad overview of Still’s disease pathogenesis and evolving therapy. (onlinelibrary.wiley.com)








Members only discussions coming soon…