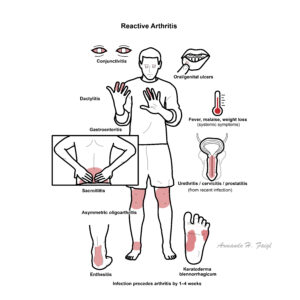
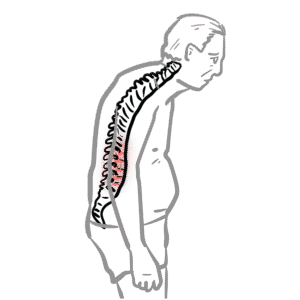
Reactive arthritis is a seronegative spondyloarthropathy that occurs after a genitourinary or gastrointestinalinfection, typically presenting as an asymmetric oligoarthritis, often with associated conjunctivitis and urethritis (formerly Reiter’s syndrome). It most commonly affects young adults aged 20–40 and shows a strong association with HLA-B27. Incidence is estimated at 30–40 per 100,000, with higher rates in HLA-B27–positive individuals following infection.
Definition
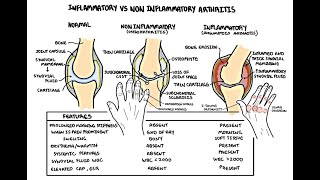
Reactive arthritis: Sterile inflammatory arthritis occurring 1–6 weeks after infection. Seronegative spondyloarthropathy: Group of inflammatory arthritides negative for RF/anti-CCP. Enthesitis: Inflammation at sites of tendon/ligament insertion. Dactylitis: Diffuse swelling of an entire digit due to synovitis and tenosynovitis.
Anatomy and Physiology
Aetiology and Risk Factors
Infectious triggers (precede arthritis by ~1–4 weeks):
No dedicated ReA classification criteria. Often diagnosed clinically based on: – Acute oligoarthritis – Preceding GI/GU infection – Absence of live pathogen in joint fluid
Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol. 2011;25(3):347–357.
Colmegna I, Cuchacovich R, Espinoza LR. HLA-B27-associated reactive arthritis: pathogenetic and clinical considerations. Clin Microbiol Rev. 2004;17(2):348–369.
Braun J, Kingsley G, van der Heijde D, Sieper J. On the difficulties of establishing a consensus definition of reactive arthritis. J Rheumatol. 2000;27(10):2185–2187.
Carter JD, Hudson AP. Reactive arthritis: clinical aspects and medical management. Rheum Dis Clin North Am. 2009;35(1):21–44.


















Discussion