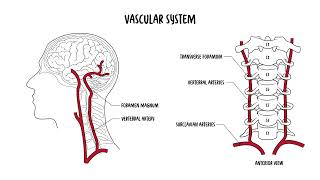
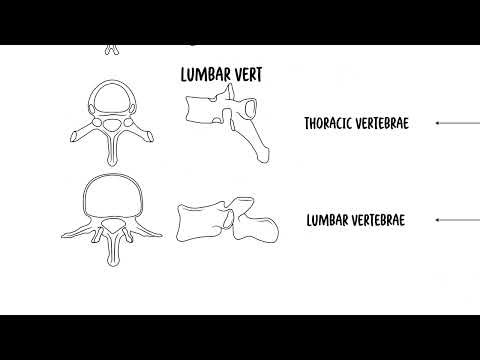
0:00 The cervical spine consists of seven vertebrae, C1 to C7, forming the uppermost 0:17 part of the 0:17 vertebral column. 0:19 It supports the skull, protects the spinal cord and allows for a wide range of 0:24 motion. 0:24 A typical cervical vertebra has several distinguishing features that 0:28 differentiate it from the thoracic 0:29 and lumbar vertebrae. 0:32 We are going to focus on the cervical vertebra C3 to C7 and look at their 0:37 distinguishing 0:38 features. 0:43 You have the vertebral body, which is the oval, small-shaped anterior portion 0:47 of the vertebra. 0:48 You have the vertebral foramen, a large triangular opening in the center, which 0:53 houses the spinal 0:54 cord and meninges. 0:57 The transverse processes are bony projections on either side of the vertebra 1:01 containing 1:02 the transverse foramina, which allow the passage of the vertebral arteries and 1:07 veins. 1:07 This is a unique feature to cervical vertebrae. 1:12 The spider's process is bifid, it split projections on the posterior side of 1:18 the vertebrae, and 1:20 it serves as an attachment site for muscles and ligaments. 1:24 Then you have the superior and inferior articular processes. 1:28 These are your facet joints that allow movement between the adjacent vertebrae. 1:34 Onsenate processes are small upward projections on the lateral edges of the 1:38 vertebral body, 1:39 which help stabilize the cervical spine by limiting excessive lateral movement. 1:49 Those are the distinguishing features of the cervical vertebrae, C3 to C7. 1:56 But what about C1 and C2? 2:00 C1 is your atlas and C2 is your axis, and these are specialized vertebrae with 2:08 distinct 2:09 structures that allow for significant head movement. 2:13 The C1, your atlas, is the first cervical vertebra, known as mentioned as the 2:21 atlas. 2:22 It supports the skull and articulates with the occipital bone at the atlanta 2:27 occipital 2:28 joint. 2:29 This joint enables the head's nodding motion, the yes movement. 2:33 The atlas lacks a vertebral body and instead has anterior and posterior arches. 2:41 C2 is the second cervical vertebrae. 2:46 This is also known as axis, and it has a unique dens, which is a adontoid 2:54 process, 2:55 which extends upward and articulates with the atlas C1. 3:00 This pivot joint allows rotation movement, the no movement of the head. 3:07 So, the atlanta occipital joint, C1 to the occipital bone, allows for nodding, 3:13 yes movement, 3:15 C1 to C2 allows for a pivot, so no movement of the head. 3:22 Let's look at some key ligaments of the cervical spine. 3:28 There are several important ones that help provide stability and support to the 3:34 spine. 3:34 You have the anterior longitudinal ligament that run along the front of the 3:38 vertebral 3:39 body and prevents hyper extension of the neck. 3:43 Posterior longitudinal ligament, located along the back of the vertebral bodies 3:47 inside the 3:47 spinal canal, it prevents hyperflection and supports the intervertebral discs. 3:53 The ligamentum flavum, a strong elastic ligament that connects adjacent lemony 3:58 and help maintain 3:59 an upright posture. 4:01 The interspinous ligaments connecting spinous processes, you have the ayla and 4:06 transverse 4:06 ligaments, and these are special in that they stabilize the dens, the adontoid 4:11 process 4:12 of the axis and allow for controlled rotation of the head. 4:17 The apical ligament joins the apex, the tip of the dens of C2 to the foramen 4:25 magnum. 4:27 So, we talked about the movements of the cervical spine, but let's talk about 4:33 it once again. 4:35 The cervical spine has the greatest range of motion in the vertebral column, 4:39 allowing 4:40 for a variety of head and neck movements. 4:43 You have flexion and extension, primarily occurring at the C0C1, the atlanto 4:49 occipital 4:50 joint, allowing the head to nod forward and backward, the yes motion. 4:56 Then you have rotation, mainly occurring at the C1 to C2, the atlanto axial 5:02 joint, enabling 5:04 the head to turn side to side. 5:06 This is your no movement of the head. 5:09 Then you have lateral flexion, which is side bending, and this happens through 5:13 the cervical 5:14 spine, but is most prominent in the mid cervical vertebra, C3 to C7. 5:26 From important anatomical relationships, the spinal cord runs through the verte 5:30 bral foramen 5:31 of the cervical vertebra. 5:33 The cervical spinal nerves is C1 to C8, not C7, it's C8, and exits through the 5:40 interval 5:41 foramina to supply motor and sensory innervation of the neck, shoulders, arms, 5:46 and diaphragm. 5:47 The phrenic nerve, which is C3 to C5, helps control the diaphragm and origin 5:53 ates in the 5:53 cervical spine, damage to this area can cause respiratory dysfunction obviously 6:04 . 6:04 How about the relationship to the vascular system? 6:07 Well, we talked about the vertebral arteries, which actually arise in the subcl 6:11 avian arteries 6:12 and passes through the transverse foramen of C6 up to C1 and enters the skull 6:18 through 6:19 the foramen magnum to supply the brainstem and posterior brain. 6:27 Compression of the vertebral arteries, such as in vertebra, bazzle, and su 6:31 fficiency, can 6:31 cause dizziness, balance issues, and transit ischemic attacks. 6:37 The internal jugular veins and chronic arteries run parallel to the cervical 6:41 spine within 6:42 the crowded sheath, supplying the brain and draining blood from the head. 6:52 Let's look at some clinical anatomy now. 6:55 You have something called cervical spondylosis and degenerative disc disease. 7:01 Survival spondylosis refers to age-related osteoarthritic changes to the 7:06 cervical spine, 7:07 including disc degeneration and bone spur formation. 7:11 It causes neck pain, stiffness, and often radiculopathy, which is when you get 7:17 irritation 7:18 of the nerves that come out of the cervical spine. 7:22 If spinal cord compression occurs, it may lead to cervical myelopathy, a 7:25 serious condition 7:26 affecting movement and coordination. 7:30 Degenerative disc disease is common age-related condition, in which the 7:35 interval discs lose 7:36 hydration and elasticity, and essentially becomes compressed. 7:45 So, cervical radiculopathy is also known as a pinched nerve, and occurs when 7:50 the nerve 7:51 roots in the cervical spine are compressed. 7:55 Usually due to herniated disc or bone spurs, it most commonly affects the C5 to 8:02 C7 nerve 8:02 roots, causing neck pain, arm pain, numbness, and weakness in the affected 8:08 nerve distribution. 8:10 And this here, I'm drawing an example of a person with a C5 radiculopathy on 8:18 one side 8:19 of the body, and it causes a specific dermatological distribution and may also 8:24 cause weakness to 8:25 wear that nerve actually supplies. 8:34 Survival myelopathy is caused by spinal cord compression. 8:39 It's different to cervical radiculopathy. 8:42 Here you typically get severe cervical spondylosis or stenosis, compressing 8:47 against the spinal 8:49 cord. 8:50 When this happens, symptoms can include gait disturbances, balance issues, hand 8:55 weakness, 8:55 and clumsiness. 8:56 It is a progressive condition often requiring surgical decompression to prevent 9:01 worsening 9:02 neurological symptoms. 9:10 Next whiplash injury. 9:11 Whiplash injury occurs due to sudden hyperflection and hyper extension of the 9:18 neck, commonly 9:19 seen in motor vehicle accidents. 9:22 This can lead to a number of injuries, including injury to ligaments, muscles, 9:26 and in rare 9:27 cases the spinal cord. 9:35 The atlanto axial instability. 9:38 This refers to excessive movement of C1 and C2 vertebrae, the atlas and the 9:45 axis, and 9:46 is often due to ligamentous laxity or trauma. 9:51 It is commonly seen in conditions such as rheumatoid arthritis and down 9:55 syndrome. 9:56 Remember there are three important ligaments around here. 9:59 The transverse ligaments is the most important stabilizer. 10:03 You have the apical ligament and the ailer ligaments. 10:07 The functional result of the joint is twofold, providing support for the occip 10:12 ut and providing 10:13 the greatest range of motion and flexibility possible while maintaining 10:19 stability. 10:20 So if there is instability, this may lead to complications such as a spinal 10:25 cord compression. 10:27 Finally, cervical fractures. 10:35 Fractures of the cervical spine can occur due to trauma, falls, or high impact 10:39 injuries. 10:40 Some very important cervical fractures include the jevisense fracture, which is 10:45 a C1 birth 10:46 fracture. 10:47 This occurs due to axial compression such as a diving accident leading to 10:53 fracture of 10:54 the atlas because it is a compression injury. 10:58 Hangman's fracture is a C2-pause interarticularis fracture. 11:04 This is a fracture through the pause interarticularis of C2, typically seen in 11:09 high impact trauma. 11:11 It is called the hangman's fracture because possibly when someone hangs 11:15 themselves, this 11:16 could be a result of it. 11:19 Then you have an odontoid or dense fracture of C2. 11:24 This is a fracture of the dense, which can cause instability and potentially 11:29 spinal cord 11:30 injury. 11:36 So in summary, we talked about the cervical spine, which consists of seven 11:40 vertebrae forming 11:41 the uppermost of the vertebral column. 11:44 We talked about the atlas and the axis, which is C1 and C2, which are very 11:50 unique because 11:51 this particular joint allows for rotation of the neck. 11:56 You have the occiput and atlas joint, which allows for the nodding of the neck. 12:02 As well, we talked about some clinical anatomy, including spondulosis and 12:05 different types 12:06 of fractures. 12:07 Thank you for watching. 12:14 [end of transcript]