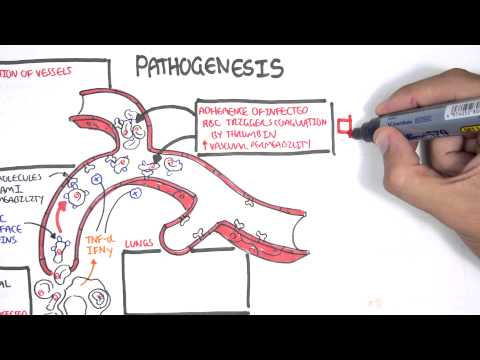
0:00 In this video we're going to talk about amebiasis. Amebiasis is a parasitic 0:10 infection 0:11 caused by intameba histolytica. Intameba histolytica infection is common 0:17 worldwide and 0:19 it can affect anyone, although it is more common in people who live in tropical 0:23 areas 0:24 with poor, sanitary conditions. Several protozoan species in the genus intameba 0:32 colonize 0:32 humans, but not all of them are associated with disease. Intameba histolytica 0:39 is well 0:40 recognized as a pathogenic ameba, associated with intestinal and extra 0:46 intestinal infections. 0:49 Other morphologically identical ameba species include intameba dyspah, intameba 0:58 moschkovsky, 1:00 and intameba bangladeshi, and these are not generally associated with disease. 1:08 The life 1:09 cycle and transmission of intameba histolytica. Intameba typically exists in 1:16 two forms, cysts 1:18 and triphozoites. The cysts forms are able to survive in the environment, and 1:24 it is this 1:25 form that is typically ingested by humans. Triphozoites are the active and 1:33 invasive form 1:34 of the parasites once in the intestine. Cystantrophozoites are typically passed 1:43 in feces. 1:44 Intameba histolytica occurs via ingestion of mature cysts, from fecally 1:51 contaminated 1:52 foods, water or hands. Therefore, the mode of transmission of the infection is 1:57 fecal 1:58 and oral root. Cysts enter the gastrointestinal tract into the small intestine. 2:05 Excystation 2:06 occurs in the small intestine, and triphozoites are released, which migrate to 2:12 the large intestine. 2:13 Triphozoites may remain confined in the intestinal lumen, and this is called a 2:19 noninvasive infection. 2:21 Here, individuals continue to pass cysts in their stool and become what's 2:27 called asymptomatic 2:28 carriers. Triphozoites can also invade the intestinal mucosa. This is called 2:36 intestinal 2:36 disease, causing conditions such as colitis, inflammation of the bowel. The tri 2:43 phozoites 2:44 here damage the mucosal layer of the intestine through several mechanisms. For 2:50 example, they 2:50 can secrete things such as protonases. They cause lysis of target cells via a 2:57 contact-dependent 2:58 mechanism. They induce apoptosis, programmed cell death. They also form what's 3:04 called 3:05 amoebopause, resulting in cytolysis of the infected intestinal cell. 3:14 Triphozoites can also invade the blood vessel, reaching extra intestinal sites 3:19 such as the 3:20 liver, brain and lungs. This is termed extra intestinal disease. It does this 3:27 because the 3:27 triphozoites are able to enter the bloodstream. They will first enter the liver 3:32 via what's 3:33 called the portal vein, and can cause a liver abscess. If the liver abscess 3:39 grows and invades 3:41 ruptures into the plural of the lung, which is right above the liver, it can 3:45 cause pluripalmonary 3:46 infection. Other sites the triphozoites can invade include the brain and the 3:52 heart, typically 3:53 via rupturing of the liver abscess here into the pericardium. 4:00 So in summary, intameba histolytica causes a range of clinical disease, 4:05 including non-invasive 4:07 infection, intestinal disease and extra intestinal disease. In the large intest 4:14 ines, the triphozoites 4:15 multiply by binary fission and produce cysts, termed end cystation, and both 4:23 stages are 4:24 passed in the feces. As mentioned, cysts can survive days to weeks in the 4:30 external environment 4:31 and remain infectious in the environment due to the protective coating it has. 4:37 Triphozoites 4:38 on the other hand cannot survive outside the human body, and if ingested, would 4:43 not survive 4:43 exposure to the gastric acidity. 4:50 Intestine symptoms of intameba histolytica infection, well the majority of int 4:55 ameba infection 4:56 are asymptomatic, about 90%. If a person has intestinal infection or intestinal 5:04 amoebia 5:04 aces, it usually occurs over 1 to 3 weeks. Symptoms include mild diarrhea to 5:11 severe 5:12 dysentery, producing abdominal pain, diarrhea and bloody stools. Complications 5:18 of intestinal 5:19 amoebia aces include forminant colitis, with bowel necrosis, which can lead to 5:27 perforation. 5:28 Perforation of the colon will cause peritonitis, with severe abdominal pain. 5:34 Toxic mega colon 5:35 can occur, which is extreme dilatation and inflammation of the colon, the large 5:42 bowel. 5:43 For extra intestinal disease, the symptoms depends on where the problem is. If 5:48 it is 5:48 a hepatic abscess, this will cause right upper quadrant pain, fever and anore 5:56 xia. Complications 5:57 of a hepatic abscess include rupturing of the abscess. If the abscess ruptures, 6:02 it can 6:03 lead to peritonitis, with severe abdominal pain. If the abscess ruptures into 6:08 the plural 6:09 of the lungs, it can cause pleuropulmonary infection, causing right upper quad 6:13 rant pain, 6:14 cough, hematosis and dyspnea. Diagnosis of amoebia aces involve a fecal 6:24 microscopy culture sensitivity, with antigen testing of the feces or PCR of the 6:32 feces. Stool 6:33 culture will not differentiate the pathogenic versus non pathogenic intermebia 6:40 species. 6:42 Antigen testing of the feces and PCR of the feces are more sensitive and can 6:47 distinguish 6:48 between intermebia histolytica and other non pathogenic intermebia species. 6:57 Treatment 6:57 of amoebiaces. For all infections, whether asymptomatic or symptomatic, paramo 7:05 myosin 7:06 is used to eliminate the cysts. For symptomatic infections such as intestinal 7:11 or extra intestinal 7:13 amoebiaces, metronidazole is used, either oral for mild infection or for more 7:19 severe 7:19 infection, intravenous metronidazole is used. So in summary, amoebiaces is a 7:26 parasitic infection 7:27 caused by intamebia histolytica. The clinical presentation varies, including 7:34 mainly asymptomatic 7:35 infections or intestinal and extra intestinal infections. Treatment involve 7:43 elimination 7:44 of the cysts with paramo myosin and for symptomatic infection, the use of met 7:50 ronidazole. Thank you 7:51 for watching. 8:05 .