Anklylosing Spondylitis (AS)
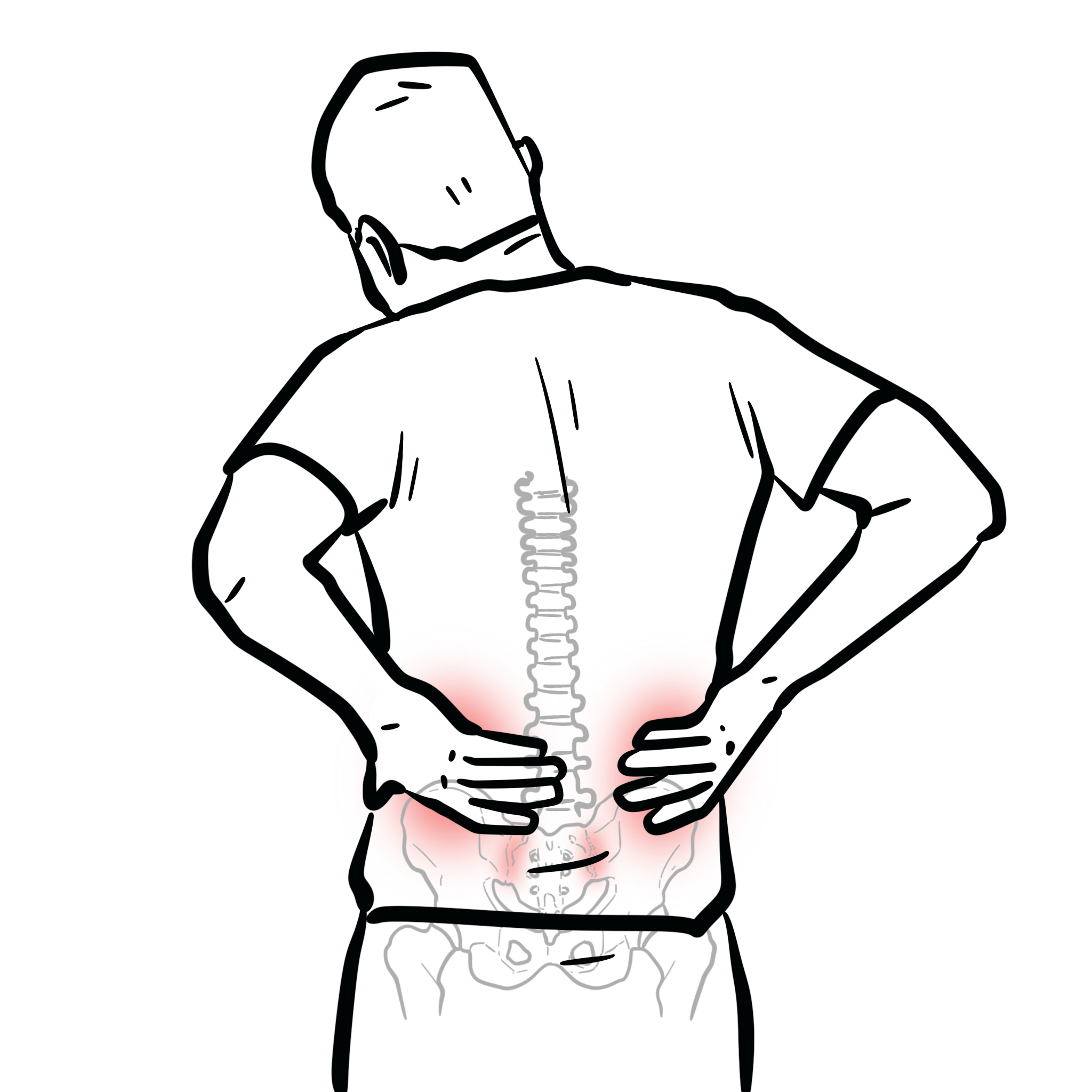

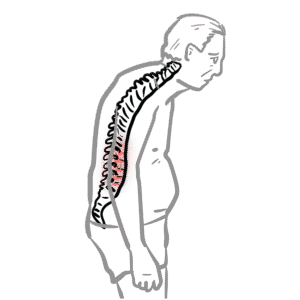
Ankylosing spondylitis (AS) is a chronic, progressive inflammatory arthritis that primarily affects the axial skeleton, especially the sacroiliac joints and spine. It is a subtype of the seronegative spondyloarthropathies and is characterised by inflammatory back pain, morning stiffness, and eventual spinal fusion in severe cases. AS often presents in young adults, typically males, and is strongly associated with the HLA-B27 genetic marker. Early diagnosis and treatment are essential to prevent irreversible spinal ankylosis and improve quality of life.
Spondyloarthritis: A group of inflammatory rheumatic diseases with shared features, including axial and peripheral arthritis, enthesitis, and association with HLA-B27.
Enthesitis: Inflammation at the site of tendon or ligament insertion into bone; a hallmark feature of spondyloarthropathies.
Bamboo spine: Radiographic appearance of the spine in advanced AS, resulting from syndesmophyte formation and vertebral fusion.
HLA-B27: A genetic antigen associated with increased risk of spondyloarthritis, particularly AS; present in up to 90–95% of AS patients.
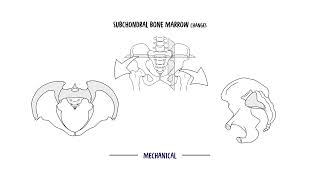
The sacroiliac joints are diarthrodial joints between the sacrum and ilium, supported by strong ligaments. In AS, they are the earliest sites of inflammation. The spinal vertebrae are connected by intervertebral discs and zygapophyseal joints, allowing for flexibility and movement. Inflammation in AS leads to new bone formation and fusion.
The entheses (attachment sites of ligaments/tendons to bone) are prone to inflammation in AS, leading to pain and eventual ossification.
The key affected structures in AS are sacroiliac joints, spine, and entheses. Usually it begins in the SIJ and moves up.
Inflammation drives both destruction and abnormal new bone formation, leading to pain and rigidity.
Inflammatory back pain improves with exercise but not with rest — opposite of mechanical back pain.
The Modified New York Criteria (1984) are the most widely used classification criteria for radiographic ankylosing spondylitis. To diagnose ankylosing spondylitis requires radiological criterion PLUS at least one clinical criterion.
| Grade | Description |
| 0 | Normal sacroiliac joints |
| 1 | Suspicious changes: possible sclerosis or minimal joint space irregularity |
| 2 | Minimal abnormality: definite sclerosis, erosions, joint space widening or narrowing |
| 3 | Moderate abnormality: marked sclerosis, erosions, joint space narrowing, partial ankylosis |
| 4 | Severe abnormality: complete ankylosis of the sacroiliac joint |
The association of HLA-B27 with AS is well established and occurs in 85–90% of patients. HLA-B27 is seen in 5–15% of the general population, with some variability associated with ethnic background, but only 5% of HLA-B27 positive people develop AS.
| Region | Early Findings | Late Findings |
| Sacroiliac joints | – Pseudo-widening of joint space – Subchondral erosions – Sclerosis (especially iliac side) | – Joint space narrowing – Ankylosis (fusion) – Loss of cortical margins |
| Spine | – Vertebral body squaring – Shiny corner sign (Romanus lesion) – Erosions at vertebral corners | – Marginal syndesmophytes – Bamboo spine (vertebral fusion via syndesmophytes) – Ossification of spinal ligaments (anterior longitudinal ligament) |
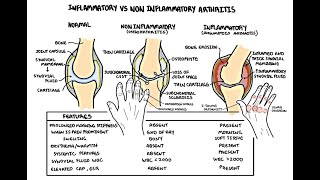
Differential diagnoses:

| Feature | Ankylosing Spondylitis (AS) | Non-Radiographic Axial Spondyloarthritis (nr-axSpA) |
| Definition | Radiographic sacroiliitis (Modified New York Criteria) on X-ray | Normal X-ray; MRI evidence of active sacroiliitis and/or HLA-B27 positivity with SpA features |
| HLA-B27 positivity | ~90% | ~70–90% |
| Gender distribution | Predominantly male | More balanced or female predominant in some cohorts |
| Progression risk | May progress to spinal fusion (bamboo spine) | ~10–30% may progress to radiographic AS over time |
| Treatment approach | NSAIDs, TNF inhibitors, IL-17 inhibitors | Same treatment principles as AS; biologics used if active disease persists despite NSAIDs |
MRI allows diagnosis before structural damage occurs — critical for early treatment.
Exercise is not just adjunct — it is cornerstone therapy in AS.
Prognosis improved with early biologic therapy and exercise.
Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.













Discussion