Dizziness and vertigo


Dizziness is a broad term used by patient to describe a range of sensations that include vertigo, presyncope, imbalance sensation and light-headedness. Vertigo describes a spinning sensation but sometimes a sensation of falling or pitching. Presyncope is a result of decrease global perfusion to the brain resulting in near fainting sensation (syncope is a transient loss of consciousness due to decrease perfusion to brain). Sensation of imbalance describes dysequilibrium and is usually of a central cause such as the brain and brain stem. Patients and with mental health can also describe a sensation of light-headedness often as a result hyperventilation or emotion stress.
| Remember Vertigo is not only caused by pathology in the vestibular system but can also be caused by cerebellar and neurodegenerative disorders. |
| Categories of dizziness | Pathophysiology | Aetiology |
| Vertigo (Spinning sensation) | Vestribular pathology | Vestibular neuritis Labyrinthitis Meniere’s disease |
| Presyncope (fainting sensation) | Reduced cerebral perfusion | Neurocardiogenic syncope Situational syncope Carotid sensitivity Postural hypotension |
| Dysequilibrium (imbalance sensation) | Gait disorder | Myelopathy Peripheral neuropathy Parkinson’s disease |
| Light-headedness (sensation of disconnection from the environment) | Psychological disorder | Anxiety Depression |
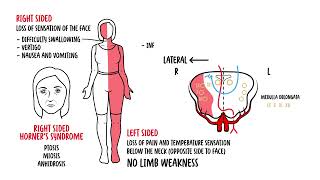
Vertigo is sensation of false movement, generally described as rotation or spinning sensation. It is caused by asymmetry of neural activity between the right and left vestibular nuclei located in the brainstem. Bilateral damage does not cause vertigo. Essential to determine if the vertigo is central or peripheral since cerebellar infarction/haemorrhage can present as vertigo and can be life-threatening.
| Remember Vertigo describes a spinning sensation but sometimes a sensation of falling or pitching. Presyncope is a result of decrease global perfusion to the brain resulting in near fainting sensation. |
Peripheral causes of vertigo (suggest inner ear pathology)
Central causes of vertigo
| Peripheral features | Central features |
| Vertigo improves with visual fixation | Vertigo does not improve with visual fixation |
| Hearing loss | Ataxia |
| Tinnitus | Visual field loss |
| Aural fullness | Diplopia |
| Positive impulse test | Limb weakness |
| Unidirectional horizontal nystagmus | Dysarthria |
| Dysphagia | |
| Nystagmus all directions (especially vertical nystagmus and horizontal nystagmus that changes direction with gaze) |
Differential diagnosis of acute vertigo
Differential Diagnosis of recurrent acute vertigo
History
| Seconds | Minutes-Hours | Days |
| Benign paroxysmal positional vertigo | Meniere’s Disease | Brainstem or cerebellar infarction |
| Perilymph fistula (trauma) | Vestibular migraine | Labyrinthitis |
| TIA | Multiple sclerosis | |
| Vestibular neuritis |
| Remember Poor pursuit or inaccurate saccades usually indicate central pathology. |
| Remember all patients suspected of central cause should get a CT and better MRI scan. |
Depends on the cause of vertigo but can include:












Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion