Overview
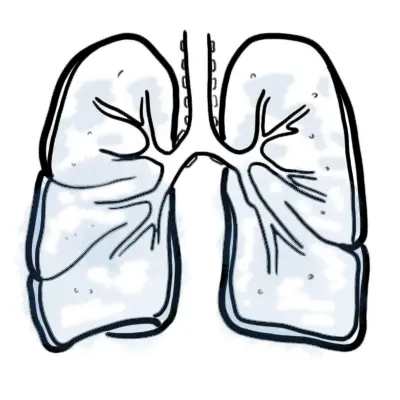
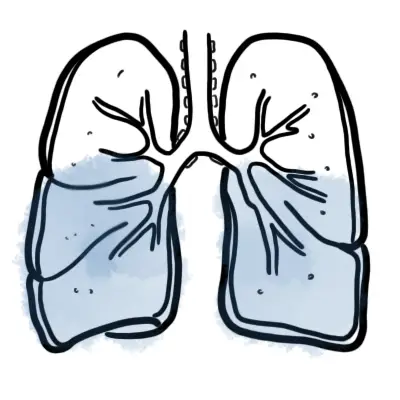
Overview ARDS is an acute, diffuse, inflammatory lung injury that leads to increased pulmonary vascular permeability, increased lung weight, and a loss of aerated tissue. Clinical hallmarks of ARDS are hypoxemia and bilateral radiographic opacities, while the pathological hallmark is diffuse alveolar damage.
Signs and Symptoms
Clinical Presentation
- 6 to 72 hours of an inciting event and worsen rapidly
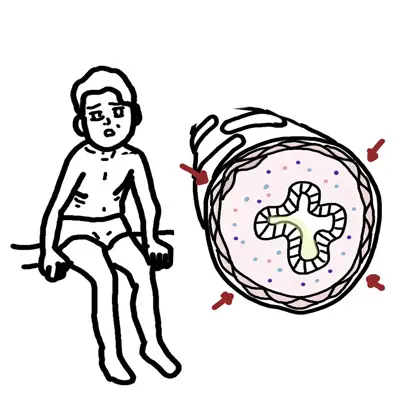
- Tachypnoea
- Tachycardia
- Diaphoresis
- Accesory muscle use
- Dyspnea
- Cyanosis (hypoxemia)
- Diffuse crackles
- +/- Cough and chest pain
| Remember Clinical hallmarks of ARDS are hypoxemia and bilateral radiographic opacities, while the pathological hallmark is diffuse alveolar damage. |
Clinical Course
- The first several days of ARDS are characterized by hypoxemia requiring a moderate to high concentration of inspired oxygen
- Most patients who survive this initial course begin to exhibit better oxygenation and decreasing alveolar infiltrates over the next several days.
- Some patients, however, have persistent, severe hypoxemia and remain ventilator-dependent. Pulmonary proliferative changes and fibrosis may progressively replace the pathological findings of diffuse alveolar damage as early as ten days after the onset of the respiratory failure.
Investigations and Diagnosis
Diagnostic Criteria – Berlin Definition
- Acute onset of symptoms of a known clinical insult (<1 week)
- Bilateral opacities consistent with pulmonary edema on Chest X-ray or CT. Other causes ruled out:
- Pulmonary nodules
- Lung collapse
- Pleural effusion
- Cardiac failure and fluid overload ruled out
- Decreased (moderate to severe) oxygenation must be present
- Mild
- Moderate
- Severe
Pathophysiology
Aetiology
- Indirect lung injury: sepsis, shock, trauma, pancreatitis, drug OD, intracranial haemorrhage, blood-transfusion related lung injury
- Direct lung injury: aspiration, inhalational injury, embolism
Pathophysiology
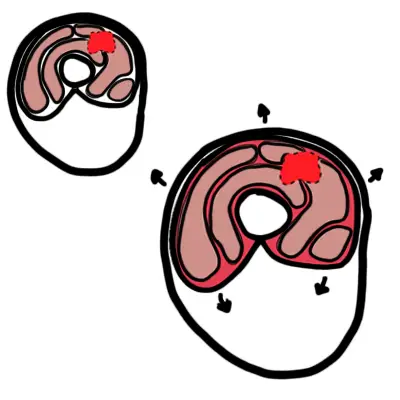
- Insult → release of inflammatory mediators promoting neutrophil accumulation in microcirculation oflung
- Neutrophils damage vascular endothelium + alveolar epithelium
- Leads to pulmonary oedema, hyaline membrane formation & difficult gas exchange
Management
- Mechanical ventilation using high PEEP & low tidal volumes to prevent ventilator-associated injury
- O2 therapy: aim PaO2>60mmHg or SpO2>90% with permissive hypercapnia
- Treat underlying disorder/precipitant
- Conservative fluid Mx strategy: aim to minimize or eliminate positive fluid balance that can → pulmonary oedema
- Supportive care
- Haemodynamic support to maintain MAP>60mmHg
- Enteral nutritional support
- DVT & stress ulcer prevention
| Side note Mortality is 30-40% and mostly from extra-pulmonary complications. |
Complications and Prognosis
Complications of ARDS
- Barotrauma
- Nosocomial infection
- Deep Vein Thrombosis
- Delirium
- Gastrointestinal ulcer
- Poor nutrition



Discussion