Overview
Fibromyalgia is a chronic, nociplastic pain condition characterised by widespread pain with prominent fatigue, sleep disturbance, and cognitive symptoms, reflecting altered central pain processing rather than tissue injury. Global prevalence is ~2–4%, higher in women, ages 20–60, and in those with mood/sleep disorders, obesity, low socioeconomic status, and comorbid rheumatic disease. Major complications include functional impairment, work disability, polypharmacy, and elevated risks of depression and suicidality; timely, multimodal, non-pharmacological care improves outcomes 2,5,15.
Definition
Nociplastic pain: pain from altered nociception without clear evidence of ongoing tissue damage or somatosensory lesion
Central sensitisation: increased responsiveness of nociceptive neurons in CNS to normal/subthreshold input, manifesting as hyperalgesia/allodynia
WPI (Widespread Pain Index): count (0–19) of painful body sites over past week used in ACR criteria
SSS (Symptom Severity Scale): 0–12 score (fatigue, waking unrefreshed, cognitive symptoms + somatic symptoms) used in ACR criteria
Classification
Chronic pain is now categorised according to the International Classification of Diseases, 11th Revision (ICD-11) into two main groups: chronic primary pain and chronic secondary pain. This classification helps distinguish pain as a disease in itself versus pain as a symptom of another condition.
Chronic Primary Pain
- Definition: Pain that persists for ≥3 months and is not better explained by another condition. It is considered a disease in its own right, often associated with emotional distress or functional disability.
- Examples
- Chronic widespread pain (CWP)
- Fibromyalgia
- Complex regional pain syndrome (CRPS)
- Chronic primary headache
- Chronic primary visceral pain (e.g., irritable bowel syndrome)
- Chronic primary musculoskeletal pain (e.g., non-specific low back pain)
Chronic Secondary Pain
- Definition: Pain that arises as a symptom secondary to an underlying disease.
- Subtypes:
- Chronic cancer-related pain
- Chronic postsurgical or post-traumatic pain
- Chronic neuropathic pain (e.g., diabetic neuropathy)
- Chronic secondary musculoskeletal pain (e.g., due to osteoarthritis or rheumatoid arthritis)
- Chronic secondary visceral pain (e.g., due to endometriosis)
- Chronic secondary headache or orofacial pain
Anatomy & Physiology
- Ascending nociceptive pathways: peripheral A-delta/C fibres → dorsal horn → spinothalamic/limbic projections → thalamus → primary/secondary somatosensory cortices, insula, ACC.
- Descending modulation: periaqueductal grey–rostral ventromedial medulla pathways inhibit/facilitate dorsal horn transmission via serotonin, noradrenaline, endogenous opioids.
- Sleep–pain interface: slow-wave sleep maintains descending inhibition; sleep loss augments temporal summation.
- Autonomic–HPA axis: sympathetic arousal and cortisol rhythms modulate pain thresholds and fatigue.
Pain intensity ≠ tissue damage; disability is driven by sensitisation, sleep and mood dysregulation.
Ask about sleep quality and exercise tolerance—changing these often shifts pain more than escalating analgesics.
Aetiology and Risk Factors
Aetiology (multifactorial, biopsychosocial)
- CNS hyperexcitability and impaired descending inhibition (nociplastic pain)
- Neuroinflammation/glial activation in pain networks (PET evidence)
- Small-fibre pathology in a subset (reduced intra-epidermal nerve fibre density)
- Dysregulated stress systems: autonomic (sympathetic overactivity) and HPA axis alterations
- Genetic/familial susceptibility with environmental triggers (infection, trauma, major stress)
Risk factors
- Female sex, middle age
- Insomnia/sleep apnoea
- Depression/anxiety
- Obesity/inactivity
- Adverse childhood experiences (PTSD)
- Catastrophizing
- Low socioeconomic status
- Comorbid rheumatic or pain disorders
- Viral illness or physical trauma as precipitant
Coexisting inflammatory disease (e.g., RA, SLE) is common—active inflammation and fibromyalgia can co-occur and amplify patient-reported disease activity.
Pathophysiology
- Predisposition (genes, sex hormones, early adversity) → heightened pain gain setting.
- Trigger (infection, trauma, psychosocial stress, poor sleep) → increased peripheral input + stress reactivity.
- CNS changes: augmented temporal summation, impaired conditioned pain modulation, altered connectivity/chemistry in insula–ACC–DMN; glial activation and pro-inflammatory signalling sustain hyperexcitability
- Systemic correlates: autonomic dysregulation (orthostatic symptoms), HPA rhythm changes, microglial cytokines, altered neurotransmitters (↓NA/5-HT; ↑glutamate)
- Clinical expression: widespread pain, sensory hypersensitivity, fatigue, sleep/cognitive symptoms; in a subset, small-fibre pathology contributes to dysaesthesias 9.
“Low phosphate” or raised CRP/ESR is not expected—abnormalities suggest an alternative or additional diagnosis.
Clinical Manifestations
- Pain: chronic (≥3 months) widespread or multisite pain, often migratory; hyperalgesia/allodynia on light pressure (e.g., trapezius, lateral epicondyle, gluteal).
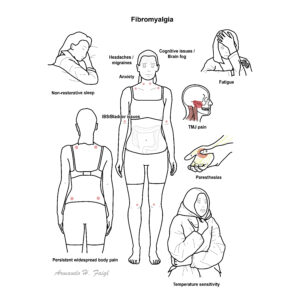
- Somatic symptoms: morning stiffness, paraesthesias, headaches/migraine, functional bowel/bladder symptoms, TMJ pain.
- Fatigue and post-exertional symptom exacerbation; non-restorative sleep, insomnia; cognitive “fibro-fog” (attention/processing speed).
- Mood: anxiety/depression common; heightened stress sensitivity.
- Autonomic: orthostatic intolerance, palpitations, thermodysregulation; sicca-like symptoms.
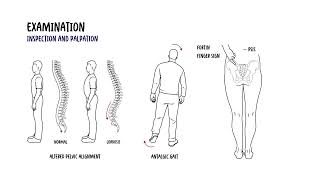
Clinical Examination
- Normal joints and neurology
- Tenderness to ~4 kg thumb pressure at multiple sites
- Normal ROM
- No synovitis
- No objective weakness.

This image series is only available to members
Triad: Widespread pain + Fatigue + Non-restorative sleep.
Tender points are not required for diagnosis since 2010/2016 ACR criteria.
Diagnosis
- 2016 ACR Diagnostic Criteria:
- WPI ≥7 and SSS ≥5 or WPI 4–6 and SSS ≥9.
- Generalised pain in ≥4 of 5 regions (jaw, chest, abdomen excluded).
- Symptoms present at a similar level ≥3 months.
- Diagnosis valid irrespective of other illnesses if criteria met.
- AAPT 2019 criteria (alternative research/clinical framework): multisite pain (≥6/9 regions), fatigue and sleep/cognitive symptoms, ≥3 months, not better explained by another disorder.
- Investigations (rule-out/minimise over-testing): FBC, TSH, CRP/ESR, CMP ± CK, coeliac serology if GI symptoms; screen for OSA when indicated; consider B12, ferritin when fatigued; autoimmune tests only if clinical suspicion of CTD
- Differential Diagnosis
- Hypothyroidism (TSH ↑, cold intolerance).
- Inflammatory rheumatic disease (objective synovitis, raised CRP/ESR, erosions).
- Myopathies (objective weakness, CK ↑).
- Small fibre neuropathy (length-dependent burning pain, reduced IENFD on biopsy).
- Chronic fatigue syndrome/ME (post-exertional malaise predominates; overlapping but distinct).
Use the Polysymptomatic Distress (PSD) score (WPI+SSS) to track severity and response.
High patient-reported activity in RA/SLE with normal inflammatory markers often reflects coexistent fibromyalgia rather than uncontrolled inflammation 2,8.
FIBRO = Fatigue, Insomnia (non-restorative sleep), Brain-fog, Regional→widespread pain, Overdetection of pain (allodynia).
Treatment
- Conservative measures
- Education
- Graded aerobic/strength exercise (land or aquatic)
- CBT or psychologically informed therapy
- Prioritise sleep optimisation
- Self-management (pacing, goal setting)
- Adjuncts (individualise): meditative movement (tai chi, yoga), mindfulness-based stress reduction, acupuncture; treat comorbidities (depression, OSA, obesity) to improve global outcomes
- Pharmacological (for severe pain/sleep disturbance after core care)
- SNRIs: duloxetine or milnacipran (pain, function).
- Pregabalin (sleep, pain); gabapentin less certain.
- Low-dose amitriptyline/cyclobenzaprine mainly for sleep.
- Avoid routine NSAIDs, benzodiazepines, and avoid strong opioids (harms outweigh benefits); tramadol only as short-term rescue in select cases.
Care delivery: shared decision-making, explain nociplastic pain model, use PSD/Patient-Reported Outcomes to track progress; de-escalate ineffective drugs.
Exercise is the most consistently effective intervention across outcomes; start low, progress slow to avoid post-exertional flares.
If multiple drugs at moderate doses fail, re-build the non-drug plan (sleep, graded activity, CBT) rather than stacking medications.
Complications and Prognosis
Complications
- Functional limitation
- Reduced QoL
- Absenteeism and work disability
- Polypharmacy
- Medication adverse effects
- Increased suicidal ideation/attempts compared with general population
Prognosis
- Fluctuating but modifiable course
- Many improve with non-pharmacological, multicomponent care
- Poorer prognosis with high baseline PSD, severe sleep disturbance, depression/anxiety, catastrophising, obesity, and persistent stressors 2,5.
Regular review to deprescribe ineffective agents and reinforce active strategies correlates with better long-term outcomes.
References
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319-329.
- Häuser W, Ablin J, Fitzcharles MA, et al. Fibromyalgia. Nat Rev Dis Primers. 2015;1:15022.
- Kosek E, Cohen M, Baron R, et al. Nociplastic pain: proposed criteria. Pain. 2021;162(11):2659-2664.
- Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Am J Phys Med Rehabil. 2016;95(9):S13-S23.
- Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR recommendations for the management of fibromyalgia: 2023 update. Ann Rheum Dis. 2023;82(9):1151-1162.
- Bidonde J, Busch AJ, Schachter CL, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst Rev. 2017;(6):CD012700.
- Bernardy K, Klose P, Welsch P, Häuser W. Efficacy of cognitive behavioural therapies in fibromyalgia: systematic review and meta-analysis. Schmerz. 2018;32(1):30-38.
- Fitzcharles MA, Nikiphorou E, Sedondi L, et al. Fibromyalgia and rheumatic diseases: diagnostic pitfalls and clinical impact. Best Pract Res Clin Rheumatol. 2019;33(3):101423.
- Grayston R, Czanner G, Elhadd K, et al. A systematic review and meta-analysis of small fiber pathology in fibromyalgia. Semin Arthritis Rheum. 2019;48(5):933-940.
- Albrecht DS, Forsberg A, Sandström A, et al. Brain glial activation in fibromyalgia — a [11C]-PBR28 PET study. Brain Behav Immun. 2019;75:72-83.
- Clauw DJ, Häuser W, Cohen SP, Fitzcharles MA. Considering the potential of centralised pain in primary care. Mayo Clin Proc. 2019;94(4):736-746.
- Arnold LM, Bennett RM, Crofford LJ, et al. AAPT Diagnostic Criteria for Fibromyalgia. Pain. 2019;160(9):1965-1973.
- Choy E. The role of sleep in pain and fibromyalgia. Nat Rev Rheumatol. 2015;11(9):513-520.
- Üçeyler N, Sommer C. Small fibre pathology in fibromyalgia: recent advances. Curr Opin Rheumatol. 2018;30(5):553-559.
- Løge-Hagen JS, Sæle A, Juhl C, et al. Suicidality in chronic pain and fibromyalgia: systematic review and meta-analysis. J Pain Res. 2017;10:2253-2263.












Discussion