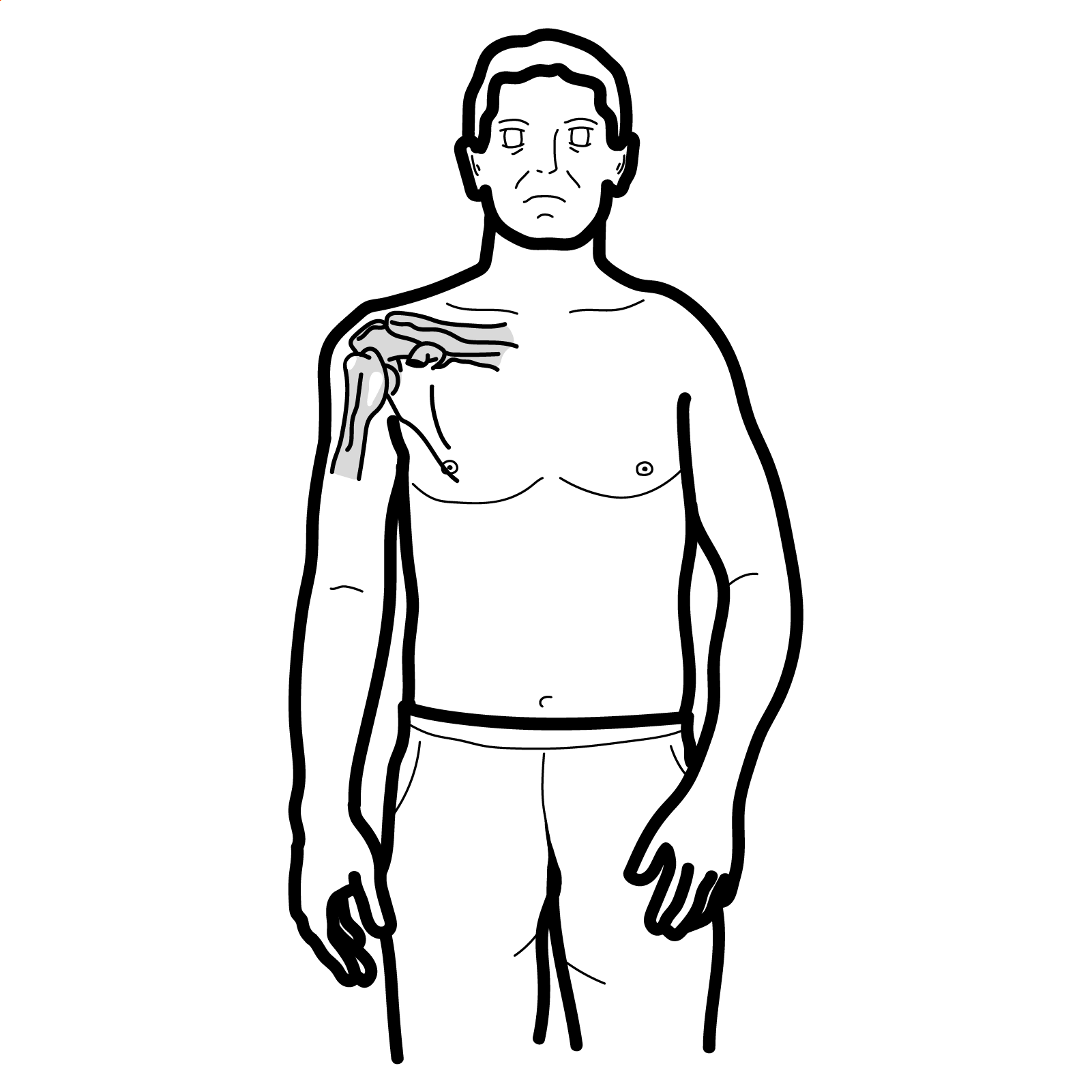
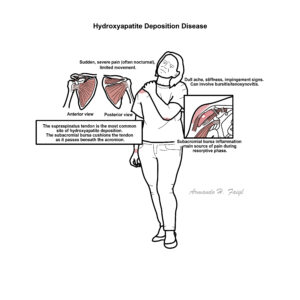
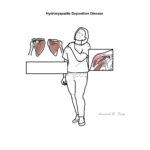
Hydroxyapatite Deposition Disease (HADD) is a crystal-induced tendinopathy caused by the deposition of hydroxyapatite (HA) crystals, typically in periarticular soft tissues, especially tendons and bursae. The shoulder (supraspinatus tendon) is most commonly affected. It often presents between ages 30–60, more frequently in women. While often asymptomatic, it can cause acute pain and functional limitation during resorptive phases.
Definition
Hydroxyapatite (HA): A calcium phosphate crystal naturally found in bone but pathologically deposited in soft tissues. HADD: Disease resulting from abnormal deposition of HA crystals in tendons or bursae, leading to pain and inflammation. Calcific tendinitis: Clinical term describing symptomatic HADD, often in the shoulder. Periarticular: Refers to structures surrounding a joint (e.g. tendons, bursae).
Anatomy and Physiology
The rotator cuff (supraspinatus, infraspinatus, subscapularis, teres minor) stabilizes the glenohumeral joint.
The subacromial-subdeltoid bursa reduces friction between the rotator cuff and overlying structures.
Tendons are poorly vascularized, especially near insertion zones (enthesis), which may predispose to crystal deposition.
Harvie P, Pollard TC, Carr AJ. Calcific tendinitis: natural history and association with endocrine disorders. J Shoulder Elbow Surg. 2007;16(2):169–173.
Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997;5(4):183–191.
Chianca V, et al. Calcific tendinopathy: imaging findings and therapeutic options. Radiol Med. 2020;125(5):431–447.
Jiménez-Martín A, et al. Calcific tendinopathy of the shoulder: clinical and radiological analysis of 100 patients. Clin Rheumatol. 2022;41(3):821–828.
de Witte PB, et al. Therapeutic options for calcific tendinitis of the rotator cuff: a state-of-the-art review. Br J Sports Med. 2016;50(15):884–890.
















Discussion