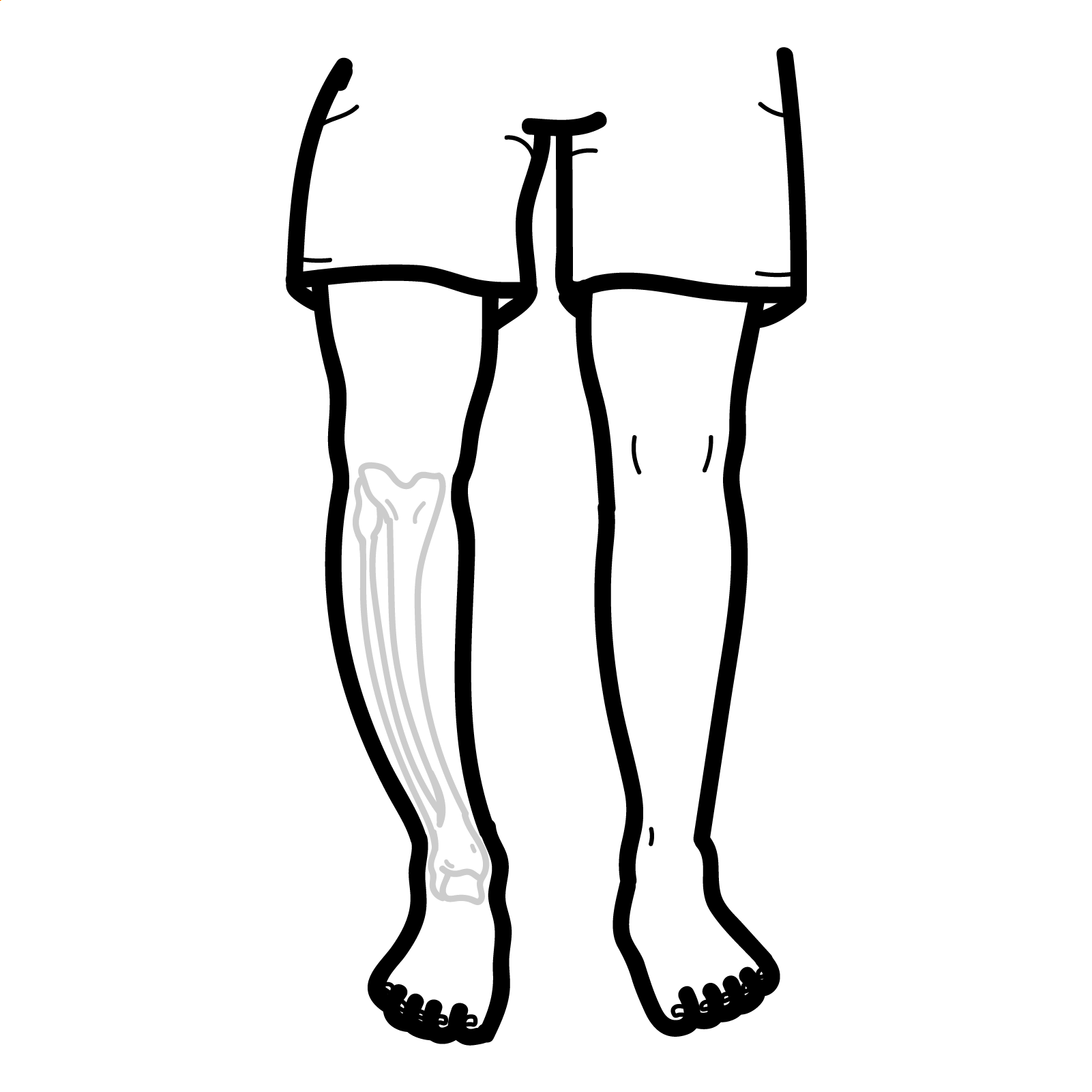
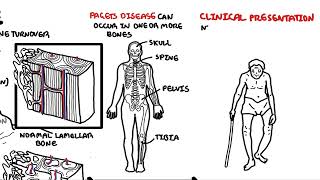
Paget’s disease of bone (PDB) is a chronic skeletal disorder characterised by focal areas of accelerated and disorganised bone remodelling. The disease begins with excessive osteoclastic bone resorption followed by a compensatory increase in osteoblastic bone formation. The result is structurally weak, enlarged, and deformed bone that is prone to fracture and complications such as arthritis or cranial nerve compression. PDB most commonly affects the pelvis, spine, skull, and long bones. It is often asymptomatic and discovered incidentally through elevated alkaline phosphatase or imaging.
Paget’s disease is the second most common metabolic bone disease after osteoporosis. It primarily affects individuals over the age of 50, with a slight male predominance. Prevalence varies by region — it is most common in people of European ancestry, particularly in the UK, New Zealand, and Australia, and is rare in Scandinavia, Asia, and Africa. The prevalence is estimated at 1–3% in adults over 55, though rates appear to be declining in some regions (1,2).
Definition
Bone remodelling: The physiological process of replacing old bone with new bone, involving both resorption (osteoclasts) and formation (osteoblasts). In PDB, this cycle is dysregulated. Alkaline phosphatase (ALP): An enzyme produced by osteoblasts during bone formation. Elevated levels in the serum reflect increased bone turnover. Mosaic pattern of lamellar bone: Histological hallmark of Paget’s disease, showing irregular cement lines due to disorganised bone formation Paget’s disease of breast: Nothing related to Paget’s disease of the bone. This is a rare type of cancer of the nipple–areola complex and that is often associated with an underlying in situ or invasive carcinoma.
Anatomy & Physiology
Normal bone remodelling involves a tightly regulated balance between osteoclastic resorption and osteoblastic formation.
PDB disrupts this balance, resulting in enlarged, brittle bones prone to deformity.
Prognosis is excellent in most cases with treatment.
The increased vascularity of bone during the osteolytic and mixed phases can divert blood flow from other tissues, potentially leading to high-output cardiac failure and symptoms such as presyncope.
Pain in Paget’s disease should be assessed to distinguish metabolic activity from complications like osteoarthritis or other musculoskeletal conditions.
References
Ralston SH, Langston AL, Reid IR. Pathogenesis and management of Paget’s disease of bone. Lancet. 2008;372(9633):155–63.
Singer FR, Bone HG, Hosking DJ, et al. Paget’s disease of bone: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(12):4408–22.
Chrzanowski W, Cundy T. Paget disease of bone. Endocrinol Metab Clin North Am. 2018;47(4):865–878.
Rea JA, Jameson KA, Compston JE. Effect of bisphosphonates on Paget’s disease: a systematic review. Bone. 2020;134:115243.


















Discussion