Paracetamol Overdose


Paracetamol overdose is a common cause of hospital presentation. Paracetamol is an analgesic and antipyretic drug used in both children and adults. Its mechanism of action is yet to be fully determined, and is likely to involve a number of pain pathways.
When taken in excess it can cause signs such as vomiting, right upper quadrant pain and altered mental status. The most serious outcome of paracetamol overdose is acute hepatic failure which could lead to death. Although hepatic injury and death is rare it is important to identify patients at risk, measure paracetamol levels using a normogram and treat accordingly. High paracetamol levels is treated with N-acetylcysteine.
Mechanism of action (not fully understood) several theories:
Metabolism Paracetamol is metabolised in the liver.
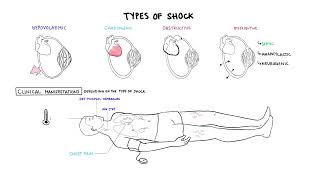
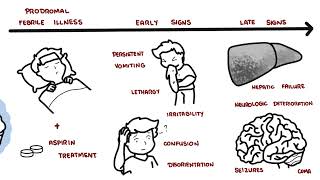
The clinical features of paracetamol toxicity is divided into 4 stages based on the time after ingestion.
Stage One – first 24 hours
Stage Two 24-48hours
Stage Three 48-72 hours
Stage Four 72hours+
Metabolism Paracetamol is metabolised in the liver.
However, when an overdose occurs, the normal metabolic pathways become saturated and more paracetamol is shunted through the P450 system increasing NAPQI levels. Too much NAPQI is toxic.
Important questions to ask in history
Acute single overdose (adult)
UB Ghaffar & Naser Ashraf Tadvi 2014, Paracetamol Toxicity: A Review
Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.














Discussion