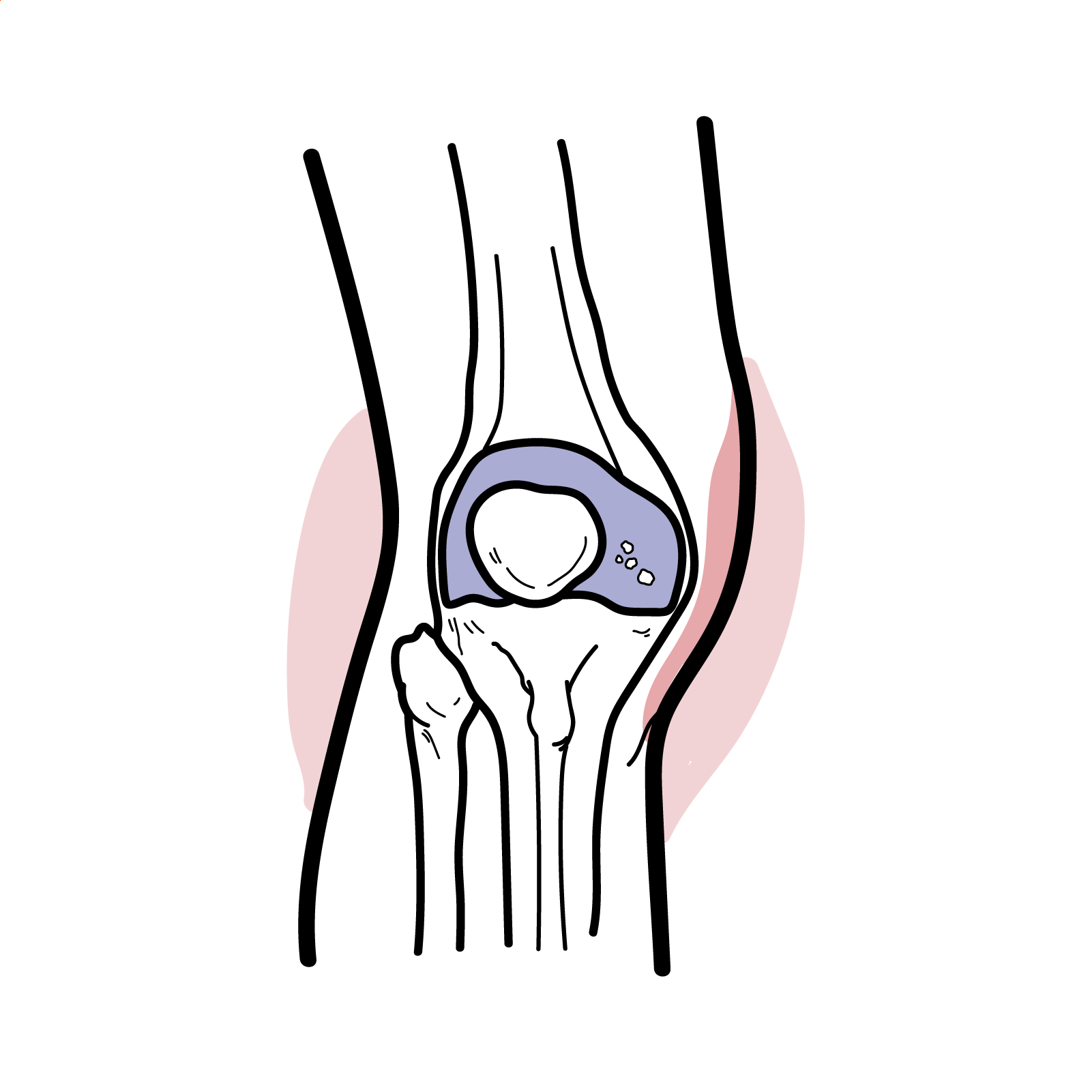
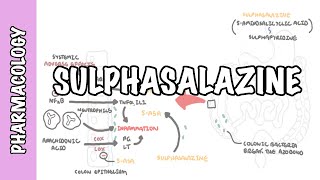
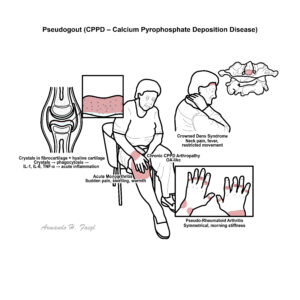
Pseudogout, more accurately known as calcium pyrophosphate deposition disease (CPPD), is a crystal arthropathy characterized by the deposition of calcium pyrophosphate dihydrate crystals in articular cartilage and soft tissues, leading to joint inflammation. It most commonly affects elderly individuals, especially over the age of 60, with a slight female predominance. Clinically, it often mimics gout or septic arthritis, and can present as acute monoarthritis or mimic chronic arthropathies like osteoarthritis or rheumatoid arthritis. The knee is the most frequently involved joint.
Definition
Calcium Pyrophosphate Deposition Disease (CPPD): A crystal arthropathy caused by the deposition of calcium pyrophosphate dihydrate crystals. Chondrocalcinosis: Radiographic finding of cartilage calcification, often associated with CPPD. Pseudogout: Acute inflammatory arthritis due to CPPD, mimicking gout clinically. Crystal arthropathy: Joint disease resulting from deposition of crystals (e.g. monosodium urate in gout, CPPD in pseudogout).
Metabolic causes of pseudogout (Young person with pseudogout) can be remembered by “4H”: Hemochromatosis, Hyperparathyroidism, Hypomagnesemia, Hypophosphatasia.
May show mild inflammatory markers elevation (ESR/CRP)
Screen for metabolic risk factors (calcium, phosphate, magnesium, iron, PTH)
Chondrocalcinosis on imaging ≠ CPPD — it can be asymptomatic.
Gout vs Pseudogout
Feature
Gout
Pseudogout
Crystal
Monosodium urate
Calcium pyrophosphate
Shape
Needle
Rhomboid
Birefringence
Negative
Positive
Most common joint
1st MTP
Knee or wrist
Age
30–50
>60
Always consider hemochromatosis in young patients with pseudogout.
Always rule out septic arthritis before confirming pseudogout.
Treatment
Acute Attack: – NSAIDs (first-line if renal function intact) – Colchicine (low-dose, especially in recurrent attacks) – Intra-articular corticosteroids if monoarticular – Systemic corticosteroids (e.g. prednisone 10–30 mg/day) for polyarthritis or NSAID intolerance
Chronic/Recurrent
Prophylactic colchicine (0.5 mg once/twice daily): no real evidence
















Discussion