Sjögren’s-Associated Interstitial Lung Disease

Sjögren’s-associated interstitial lung disease (Sjögren’s-ILD) is a significant extra-glandular manifestation of primary Sjögren’s disease (pSS), occurring in ~9–20% of patients clinically, with subclinical involvement detectable in up to 50% on HRCT. It may precede sicca symptoms or develop late in the disease course. The most common ILD pattern is nonspecific interstitial pneumonia (NSIP), followed by usual interstitial pneumonia (UIP), organizing pneumonia (OP), and lymphocytic interstitial pneumonia (LIP). Risk factors include older age, male sex, smoking, anti-Ro/SSA positivity, and high disease activity. The most important complication is progressive pulmonary fibrosis leading to respiratory failure.
Primary Sjögren’s Disease (pSS): Chronic autoimmune disorder characterized by lymphocytic infiltration of exocrine glands, leading to sicca symptoms and systemic manifestations.
Interstitial Lung Disease (ILD): Group of disorders involving inflammation and/or fibrosis of the lung interstitium.
Nonspecific Interstitial Pneumonia (NSIP): ILD pattern with uniform interstitial inflammation and fibrosis, common in Sjögren’s-ILD.
Lymphocytic Interstitial Pneumonia (LIP): Rare ILD pattern with diffuse infiltration of alveolar septa by lymphocytes and plasma cells.
Risk Factors
ILD can be the first manifestation of pSS, especially in older male patients.
Raynaud’s phenomenon, lymphopenia, and rampant dental caries have been linked to higher ILD prevalence.
LIP pattern reflects intense lymphoid proliferation, sometimes linked to lymphoma risk.
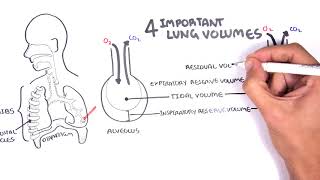
Key Investigations
Differential Diagnoses
| Condition | Differentiating Feature |
| IPF | Older age, no sicca symptoms, UIP pattern |
| Sarcoidosis | Noncaseating granulomas, hilar lymphadenopathy |
| Hypersensitivity pneumonitis | Exposure history, centrilobular nodules |
| Lymphoma | Mass lesions, monoclonal lymphoid proliferation |
| Pattern | HRCT Features | Common in Sjögren’s? | Prognosis |
| NSIP (Nonspecific Interstitial Pneumonia) | Bilateral, symmetric ground‑glass opacities ± fine reticulation; subpleural sparing common | Yes – most common | Better than UIP |
| UIP (Usual Interstitial Pneumonia) | Basal/subpleural reticulation, honeycombing, traction bronchiectasis; heterogeneous | Less common | Poorer prognosis |
| LIP (Lymphocytic Interstitial Pneumonia) | Diffuse ground‑glass opacities, thin‑walled cysts, septal thickening, scattered nodules | Characteristic but rare | Variable |
| OP (Organizing Pneumonia) | Patchy, peripheral or peribronchial consolidations; “reverse halo” sign possible | Occasional | Good with treatment |
| DAD (Diffuse Alveolar Damage) | Diffuse ground‑glass opacities, consolidation; ARDS‑like | Rare | Poor; acute presentation |
In primary Sjögren’s, NSIP is most common, LIP is characteristic but less frequent, and UIP is less common but carries a worse prognosis.
LIP may respond better to immunosuppression than fibrotic UIP.
Prognosis
















Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion