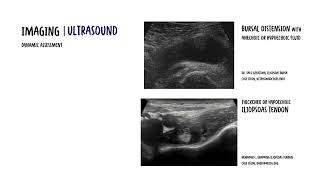
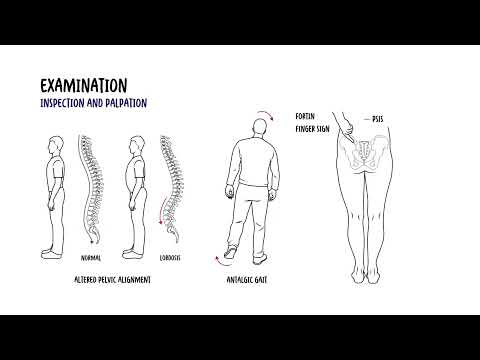
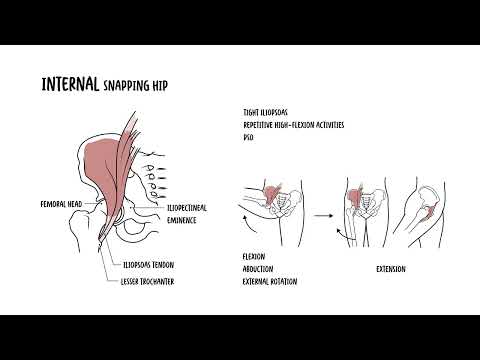
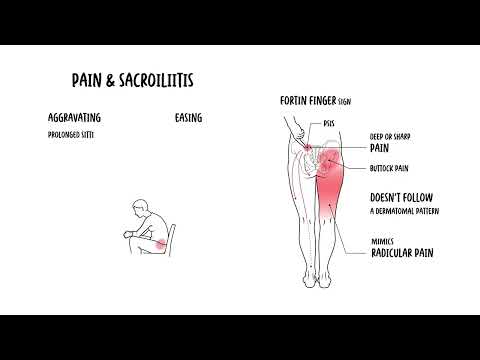
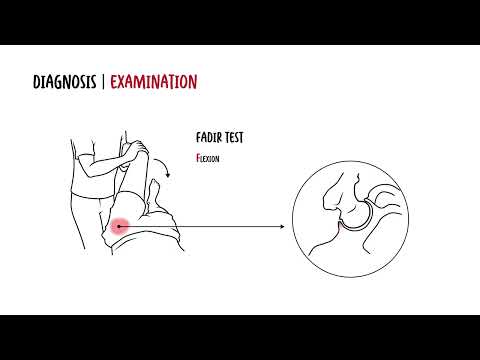
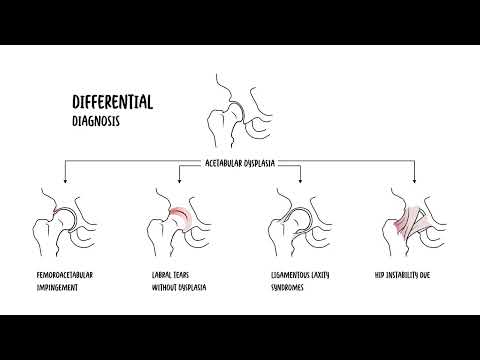
0:00 In this video, we're going to talk about Alliosaurus tendonopathy and vasitis. 0:17 So hip pain doesn't always come from arthritis or the joint itself. 0:22 Sometimes it arises from powerful muscles and tendons that move the hip joint. 0:27 One important cause is alliosaurus tendonopathy and vasitis. 0:32 Conditions that really involve the irritation of the alliosaurus tendon and the 0:37 alliosaurus 0:37 bursa, a fluid sac that cushions the tendon where it crosses the front of the 0:47 hip. 0:49 Let's revise some anatomy first. 0:51 So the alliosaurus muscle or complex is the primary hip flexor. 0:57 It's critical for walking, running and stair climbing because you flex your hip 1:02 . 1:03 The alliosaurus is formed by psoas major and the alliacus. 1:09 Psoas major originates from the lateral surface of T12 to L5 to triple bodies 1:13 and discs and 1:14 the L1 L5 transverse processes, while alliacus arises from the alliac fossa and 1:20 inner lip 1:21 of the alliacrest with small slips from the anterior sacro alliac ligaments. 1:27 The two bellies descend from the pelvis, pass beneath the inguinal ligament in 1:35 the muscular 1:35 lacuna and converge into a common tendon that inserts on the lesser trochanter 1:43 of the fema. 1:44 A thin expansion, the alliosaurus tendon slip, may blend with the femoral shaft 1:50 or hip capsule 1:52 near the pectinial eminence. 1:56 The alliosaurus bursa lies between the tendon and the anterior hip capsule, 2:03 reducing friction 2:04 during motion. 2:11 So what's the mechanism of alliosaurus tendonopathy and bursitis? 2:15 Well, tendonopathy develops from repetitive tensile and compressive loading, 2:20 with repeated 2:21 hip flexion and then extension. 2:23 The tendon undergoes microtrauma at its insertion onto the lesser trochanter or 2:28 where it glides 2:29 over the pelvic brim. 2:32 Poor load management, sudden increases in training intensity, repetitive 2:36 kicking, uphill 2:38 running, biomechanical issues such as leg length, discrepancy, excessive 2:42 anterior pelvic tilt, 2:44 hip instability, or adjacent pathologies such as labral tears, dysplasia, 2:49 amplify shear 2:51 and compressive stress that can result in tendonopathy. 2:54 Over time, this really results in tendon thickening if you have tendonopathy, 2:58 disorganization 3:00 of collagen fibers and pain. 3:09 Besitis occurs when the alliosaurus tendon irritates the underlying bursa. 3:16 Excessive friction or compressive forces lead to bursal inflammation and fluid 3:20 accumulation. 3:21 In some cases, alliosaurus bursitis communicates with the hip joint capsule, 3:27 especially in 3:28 patients with arthritis or joint defusions, which may complicate the clinical 3:33 picture. 3:34 Together, tendonopathy and beside us often co-exist, presenting as painful 3:40 anterior hip 3:42 snapping or deep groin pain. 3:51 So let's focus more on that clinical presentation. 3:56 The pain is deep anterior groin pain, sometimes radiating to the thigh or knee, 4:01 patients may 4:03 point just inside the hip crease. 4:07 Aggravating factors, because the alliosaurus complex is a primary hip flexor, 4:13 the pain 4:13 is worse with resisted hip flexion. 4:17 So for example, stairs, sit to stand, straight leg raise, or even hip extension 4:24 can aggravate 4:25 the pain. 4:26 So pushing stride, coming out of a car, sitting with a hip flex for long 4:31 periods may also 4:33 cause discomfort. 4:35 Pain may limit walking, sport and daily mobility, and severe beside us the pain 4:40 can even disturb 4:41 sleep when lying flat. 4:49 To diagnose, really history and examination are usually sufficient, key 4:53 findings include 4:54 tenderness over the femoral triangle and pain on resisted hip flexion, 15 to 30 5:02 degrees. 5:03 But you got to think about differentials such as alliosaurus, abscess or 5:07 collection that 5:08 can also cause similar findings. 5:11 There are a few dynamic tests and these dynamic tests are really to check for a 5:16 snapping internal 5:18 hip phenomenon that may occur. 5:21 So essentially you can reproduce snapping or anterior groin pain when moving 5:27 from flexion 5:28 abduction external rotation to extension adduction internal rotation. 5:35 This will cause a palpable or audible snap. 5:39 Passive hip extension, a prone or Thomas position can provoke pain and tight 5:44 ness, because you 5:45 are stretching the alliosaurus muscle. 5:54 For imaging, ultrasound is good, it's a dynamic assessment and is particularly 6:00 valuable. 6:01 You're looking for thickened or hypoechoic alliosaurus tendon, suggesting tend 6:07 inopathy, 6:08 personal distension and anechoic or hypoechoic fluid, reproduction of snapping 6:15 as the tendon 6:16 moves across the pelvic brim, peri-tendinous hypervascularity on Doppler 6:22 indicates active 6:24 inflammation. 6:25 Ultrasand is also used as modality of choice for guided bursal corticosteric 6:33 injection. 6:34 MRI is good as it provides more comprehensive evaluation of both the tendon and 6:39 other structures. 6:41 What you're looking for is tendon thickening, increased T2 stir signal within 6:46 the tendon, 6:47 which indicates tendinosis or partial tear, such as shown in this example, 6:52 fluid-filled 6:53 distension of the alliosaurus bursa, which may extend into the pelvis or 6:57 communicate 6:58 with the hip joint, like in this image. 7:02 You can also see signs of associated intra-articular pathology, such as cyanov 7:07 itis, labral tears 7:08 or contral wear. 7:10 MRI is also useful to exclude mimics or differentials, such as femoral neck 7:16 stress fracture, inguinal 7:18 hernia or pelvic pathology. 7:20 Again, I did mention it earlier, psois absus or collection can mimic pain with 7:26 hip flexion. 7:32 Now, let's talk management. 7:35 Most cases improve with non-surgical treatment. 7:39 You can divide management into conservative, interventional or surgical options 7:44 . 7:44 For conservative, rest and activity modification to reduce repetitive hip flex 7:50 ion. 7:50 Physiotherapy with a focus on stretching, the alliosaurus and strengthening 7:54 surrounding 7:55 stabilizers is important, NSAIDs or ice for pain relief. 8:01 Multiple options, ultrasound-guarded corticosteroid injection into the allios 8:05 aurus bursa can provide 8:06 diagnostic and therapeutic benefit. 8:10 There is surgical options, which is rare, but tendon release or lengthening may 8:14 be considered 8:15 in chronic refractory cases, especially if associated with snapping hip 8:22 syndrome. 8:23 I have a separate video on snapping hip syndrome that looks into the different 8:27 subtypes of 8:28 snapping hip syndrome, including this one. 8:37 The prognosis, well, the outlook is generally excellent with early recognition 8:40 and appropriate 8:41 treatment. 8:42 Most athletes and active individuals can return to full activity once the 8:46 tendon is rehabilitated 8:48 and the underlying contributing factors are corrected. 8:52 Persistent or untreated cases however may lead to chronic issues and secondary 8:56 hip pathology. 9:03 So in summary, alliosaurus tendinopathy and bursitis are important causes of 9:07 anterior 9:08 hip pain. 9:09 They result from overuse or irritation of the alliosaurus tendon and its 9:15 adjacent bursa, 9:17 leading to groin pain that worsens with hip flexion activities. 9:22 With physiotherapy, activity modification and if needed image, guided injection 9:27 . 9:27 Most patients achieve for recovery.