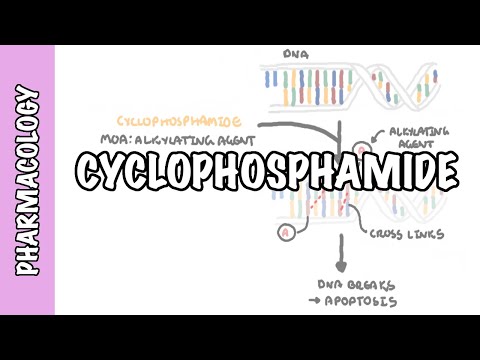
0:00 In this video, we are going to look at local anesthetics and this is sort of an 0:19 overview 0:20 on local anesthetics to do with pharmacology. 0:23 Now, local anesthetics are used in minor surgery to numb a small part of the 0:29 body. 0:30 So here you can see some doctor injecting some local anesthetics into the body 0:38 to numb 0:38 the area so we can't feel anything. 0:42 Interestingly enough, cocaine was one of the first anesthetics, actually it was 0:46 the first 0:47 anesthetics to be discovered. 0:49 We can administer anesthetics through intradermal, subcutaneous, or intrathecal 0:56 in the spine. 1:01 Before we continue on, please remember the basics of pharmacology. 1:07 If a drug is in an unionized form, it can penetrate the cell membrane, it is 1:13 effective. 1:14 For example, it can be absorbed by the body. 1:18 However, if a drug is in an ionized form, if it's polar, it cannot penetrate 1:24 the cell 1:25 membrane, it's not very effective, and for example, it cannot be absorbed by 1:30 the body. 1:31 Now, a local anesthetic is a weak base, with a pKa of about 8 and 9. 1:38 And in an unionized form, it can penetrate the cell membrane, it is quite 1:43 effective. 1:44 However, if when it enters a physiological pH, which is slightly acidic below 7 1:52 , it will 1:52 become ionized, and so it cannot penetrate the cell membrane. 2:00 So for example, if we were to administer a local anesthetic to a person 2:05 suffering from 2:06 high levels of acids in their body, the local anesthetic will be ionized very 2:11 quickly, and 2:12 so it's not very effective. 2:15 So this is an important concept to know, and we'll learn more about it during 2:21 this video. 2:22 So how do local anesthetic work? 2:24 Will they numb a small part of the body by particularly working on the nerves, 2:29 especially 2:30 the Afrid nerve fibers, the pain fibers, by preventing the pain fibers to send 2:36 pain signals 2:37 to the brain, let's have a closer look. 2:43 Here is the cell membrane of the neuron with channels. 2:49 Here is the outside of the neuron, and here is the inside. 2:54 The inside's not meant to be here, it's meant to be in the inside. 2:57 I hope you understand that. 2:59 In the inside of the neuron, it's more negatively charged in respect to the 3:05 outside. 3:06 In the inside we have more potassium ions, and in the outside we have more 3:11 sodium ions. 3:12 When an action potential or impulse travels through along the neuron, the 3:18 inside will 3:19 become more positive, like so, because of the influx of sodium ions from the 3:25 outside 3:25 to the inside. 3:30 What happens when a local anesthetic comes along? 3:32 A local anesthetic will come along in an unionized form, meaning that it can 3:37 penetrate the cell 3:38 membrane. 3:39 So here, the local anesthetic will penetrate the cell membrane and come inside 3:45 the neuron. 3:46 The inside of the neuron is slightly acidic in the physiological pH, and so 3:51 when this 3:52 local anesthetic goes inside the neuron, it will become ionized, and so will 3:58 not leave 3:59 the neuron, and this is what we want, because then the local anesthetic in an 4:06 ionized form 4:07 can bind on the sodium channels here, and essentially prevent the sodium ions 4:13 from coming 4:14 inside the neuron, and so prevent the impulse or action potential from propag 4:20 ating down 4:21 along the neuron. 4:24 So in summary, a local anesthetics essentially prevents both the generation and 4:29 conduction 4:29 of the nerve action potential. 4:32 It blocks the sodium channels by physically plugging the trans membrane port 4:37 from the 4:38 inside, and so when we prevent the conduction of this action potential from 4:45 this pain fiber, 4:47 that means that the brain will not receive this pain signal, and so we would 4:51 feel no 4:52 pain when we use local anesthetics. 4:55 However, local anesthetics actually work on every type of nerve, not only these 5:00 afferent 5:01 nerve fibers, the pain fibers, but as a general rule, they work more on smaller 5:06 fibers, because 5:07 small fibers are more susceptible than large fibers, and local anesthetics also 5:12 work particularly 5:13 on myelinated, more than unmyelinated nerve fibers. 5:19 So if we draw this up from the most susceptible to the least susceptible, is 5:20 that no-ceceptors, 5:26 the pain fibers are more susceptible to local anesthetics, and then we have the 5:31 sympathetic 5:32 fibers, the temperature fibers, and so on and so on until finally on motor 5:38 fibers, but we 5:39 would need a massive dose of local anesthetic to paralyze a person. 5:46 As a side note, let's look at another type of local anesthetic, a natural one, 5:51 which is 5:52 secreted by pufferfish, and it's a toxin. 5:57 So here again, I'm drawing the membrane of a neuron, and with the channel, the 6:04 inside 6:05 is more negative in respect to the outside, but when an action potential comes 6:09 along, 6:09 the inside will become more positive. 6:11 The pufferfish, as we know, is pretty toxic for humans, and that is why we stay 6:16 away 6:16 from it. 6:17 The pufferfish, this is because a pufferfish secretes a toxin known as tetrodot 6:22 oxin, 6:23 or TTX. 6:24 TTX, unlike our local anesthetic that we use in hospital, TTX blocks the sodium 6:30 channel 6:31 from the outside, like so, and so this will not allow sodium ions to come 6:37 inside and so 6:38 will not allow the action potential to pass through. 6:44 The side effects of using local anesthetic include headache, dizziness, 6:48 confusion, and 6:49 CNS depression, which may be fatal if it leads to respiratory depression. 6:55 However, cocaine actually doesn't cause CNS depression, but causes excitement 7:04 instead. 7:05 So that's cocaine. 7:07 What effects of local anesthetic also affect the heart? 7:10 It can lead to myocardial depression, vasodilation as well, and so care must be 7:16 taken. 7:17 We have to check the blood pressure before giving local anesthetic. 7:21 Cocaine again, on the other hand, doesn't cause myocardial depression, but 7:25 increases 7:26 like the activity. 7:28 Now, let's look at some types of local anesthetics, some popular ones. 7:33 Lignocaine, also called Lidocaine in America, is as a rapid induction, has a 7:39 medium duration, 7:41 so you won't feel pain for medium duration, has good tissue penetration, and it 7:46 's very 7:47 commonly used, especially in dentistry, I think. 7:50 But lignocaine also works as an anti-arithmic drug, a class 1B. 7:55 So this lignocaine can be local anesthetic as well as anti-arithmic drug. 8:01 As an anti-arithmic drug, it tries to fix, not fix, but tries to help in arrh 8:12 ythmias. 8:14 So it works on the depolarization phase, rapid depolarization phase of the vent 8:20 ricles. 8:21 So if this was the normal action potential of a ventricle myocyte, where we, in 8:27 the 8:27 zero phase, we have a rapid depolarization caused by an increase in sodium 8:33 influx, lignocaine 8:34 will cause this type of shift, which will essentially slow down the depolar 8:40 ization phase. 8:43 But we don't really need to know that lignocaine is an anti-arithmic drug 8:47 because this is 8:48 a local anesthetic video, but that's just a good concept to understand. 8:53 Another type of local anesthetic is procaine, which is, I wrote here, crap 8:58 because it has 8:59 many side effects and it's not very useful. 9:02 And the last local anesthetic I'm going to talk about is bupvacaine. 9:07 It has a slow onset, a long duration, and medium tissue penetration. 9:13 So it's pretty good. 9:14 And that is why it is commonly used in long surgeries because of this long 9:18 duration. 9:19 However, it has high cardiotoxicity. 9:22 So care must be taken when using this with people suffering from my hot failure 9:28 or something 9:28 like that.