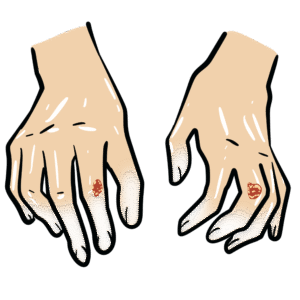
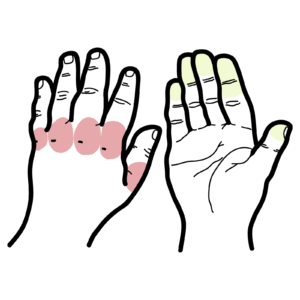
0:00 Hello, in this video, we're going to talk about Raynodes or Raynodes Phenomenom 0:11 , which 0:11 is an exaggerated vascular response to cold temperature or emotional stress. 0:17 It results in episodic abnormal vasospasm or vasoconstriction, causing a well 0:23 demarcated 0:24 color change in the skin of the digits, primarily the fingers or even the toes. 0:31 Here's an example of a well demarcated discoloration involving multiple fingers 0:35 of the hand. 0:37 In Raynodes Phenomenon, vasospasm leads to a distinct triphasic color change in 0:43 the 0:44 affected area. 0:45 Let's take a closer look at the mechanism of the color change. 0:49 So under normal conditions, you have blood supply, arterioles supplying oxygen- 0:55 rich 0:55 blood to the digits to the fingers. 1:00 In Raynodes Phenomenon, you get vasoconstriction with vasospasm. 1:05 This is typically exacerbated by cold temperature or even stress. 1:09 This results in narrowing of the blood vessels in the fingers. 1:13 The initial color change is white, also known as pallor, caused by reduced perf 1:18 usion of 1:18 blood to the area, causing the skin to blanch. 1:24 The next color change is blue, also known as cyanosis. 1:28 This occurs after some time due to the lack of oxygen being delivered to the 1:33 area. 1:33 Prolonged lack of oxygen leads to desaturation of hemoglobin in the affected 1:41 area. 1:42 The final color is red or erythema, upon reforming or resolution of the spasm, 1:48 blood 1:49 flow returns, causing a reactive hyperimia, the skin turns red. 1:55 The blood vessels typically dilates. 1:59 This is the triphasic response seen in Raynodes Phenomenon, white, blue and red 2:06 . 2:07 The fingers then eventually return to normal color again. 2:11 As mentioned, Raynodes Phenomenon is often triggered by cold exposure or 2:15 emotional stress. 2:16 It can be a benign condition or associated with more severe underlying diseases 2:23 , which 2:23 leads us to the classification of Raynodes Phenomenon. 2:26 There are two main types of classifications, primary Raynodes Phenomenon and 2:31 secondary 2:32 Raynodes Phenomenon. 2:34 Primary Raynodes Phenomenon is also known as Raynodes Disease, and this is the 2:37 most common. 2:39 There is vasospasmodic attacks triggered by cold or stress. 2:44 This is a benign form. 2:45 It occurs in the absence of any other underlying disease and generally affects 2:50 young people, 2:50 often women, typically between the ages of 15 and 30. 2:57 Secondary Raynodes Phenomenon is also known as Raynodes Syndrome, and this form 3:01 is typically 3:02 pathological and is associated with underlying diseases, most commonly 3:06 autoimmune or connective 3:08 tissue disease, such as systemic lupus erythmatosis or systemic sclerosis. 3:15 The onset of secondary Raynodes Phenomenon is typically middle to older adults. 3:21 It can occur both in females and in men, however, being male of any age with 3:27 Raynodes 3:28 should ring alarm bells for secondary Raynodes Phenomenon. 3:33 The other difference between primary and secondary Raynodes is that primary is 3:37 usually bilateral, 3:38 meaning affects both hands or feet, and often symmetrical in color change. 3:45 Whereas secondary Raynodes, the discoloration can occur in random fingers or 3:49 digits, in 3:50 any amount of digits. 3:53 Secondary Raynodes Phenomenon is more severe and can be painful. 3:57 Secondary Raynodes Phenomenon has a higher risk of complications, such as ulcer 4:01 ation of 4:02 the digits, gangrene or tissue loss. 4:06 Here's an example of a hand with secondary Raynodes Phenomenon that has 4:09 developed digital 4:10 ulceration. 4:14 Another key difference to differentiate primary to secondary Raynodes Phenomen 4:18 on is by assessing 4:20 the nail beds, looking at the nail bed capillaries, and this can be done using 4:26 a capilloscopy. 4:27 In primary Raynodes Phenomenon, there is normal nail bed capillaries, whereas 4:33 in secondary, 4:34 it is abnormal. 4:36 Let's take a look at what a normal nail fold capillary should look like. 4:45 In this diagram, you can see that the capillaries at the base of the nail bed 4:50 look like almost 4:51 like hairpin loops. 4:54 Again, this is compared to a nail bed that is seen in secondary Raynodes Phen 5:00 omenon. 5:02 Here you can see dilated, disorganized capillary loops with some associated 5:09 dropouts, so drop 5:11 out of the actual capillaries. 5:14 And again, these changes are seen using a capillaroscopy by looking underneath 5:18 the nail 5:19 bed in someone who has Raynodes Phenomenon. 5:22 The other difference between primary and secondary Raynodes is that primary Ray 5:26 nodes, you have 5:26 absent of antibodies, such as anti-nuclear antibodies, ANA, or very low titers, 5:31 whereas 5:32 secondary Raynodes, you have positive ANA, relatively high titer greater than 5:37 160, or 5:38 presence of another specific autoantibody, such as anti-centra-mere antibody. 5:47 So how do you treat Raynodes Phenomenon? 5:48 Well, the management of Raynodes Phenomenon depends on the severity, frequency 5:52 of episodes, 5:53 and whether the condition is primary or secondary. 5:57 First and foremost, lifestyle modifications. 6:00 It's important to avoid any triggers, so patients should avoid cold exposure by 6:04 wearing 6:05 warm clothing, gloves, and keeping their body temperature quite stable. 6:10 Stress management is also a very important key in reducing attacks. 6:14 Smoking cessation, nicotine is a potent vasoconstrictor. 6:17 It's also important to avoid medications that can trigger vasoconstriction, 6:22 such as decongestants 6:24 and certain beta blockers used in heart conditions can exacerbate Raynodes Phen 6:30 omenon. 6:31 Then you can use medications, pharmacological treatment. 6:35 These include calcium china blockers, phosphodiesterase inhibitors, prostacycl 6:39 ine analogs, 6:40 topical nitrates, as well as endotheline receptor antagonists, which are 6:45 typically used 6:46 in more severe cases and has been shown to reduce digital ulcer formation. 6:52 Finally, it's important to treat any underlying conditions associated with Rayn 6:56 odes Phenomenon. 6:57 This is typically, I'm talking about secondary causes or secondary Raynodes 7:02 Phenomenon, which 7:03 includes systemic lupus or systemic sclerosis, and so the use of immunosupp 7:07 ressive drugs 7:08 may be used in this situation. 7:12 In conclusion, Raynodes Phenomenon, while common, can vary greatly in severity 7:15 depending on whether 7:16 it is primary or secondary. 7:19 Primary Raynodes is generally benign, whereas secondary Raynodes may indicate 7:22 serious underlying 7:23 pathology and carries a risk of complications, such as ulcers.