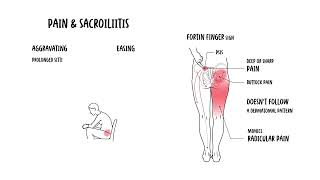
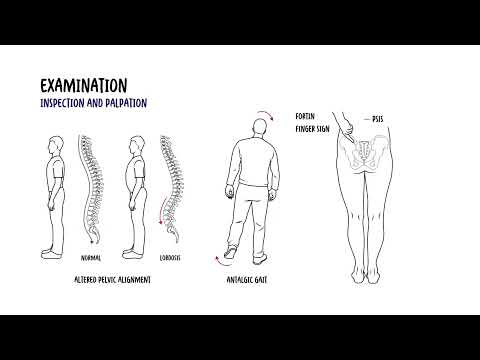
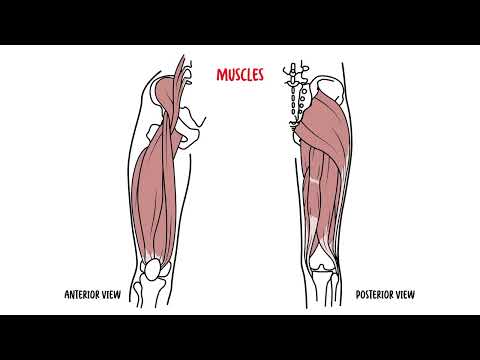
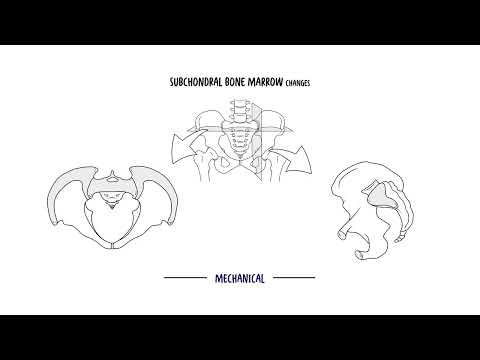
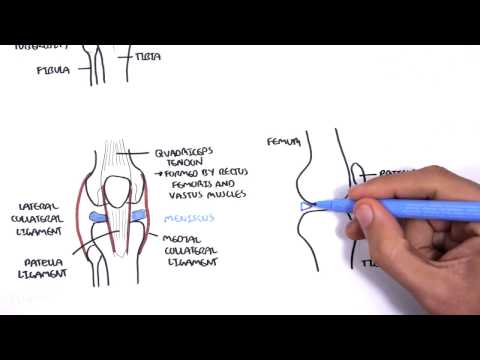
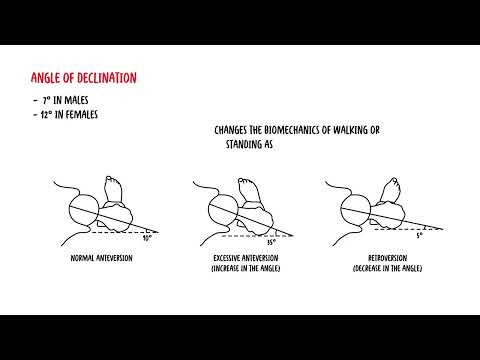
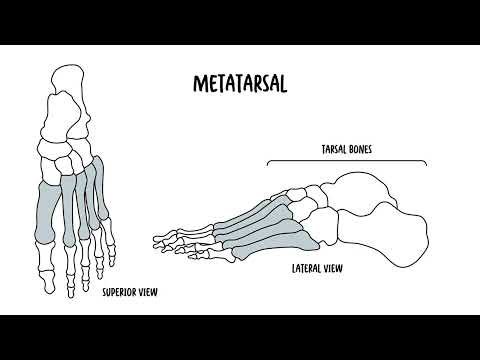
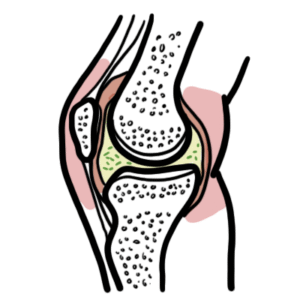
0:00 The sacroiliac joints are synovial joints, formed by the irregularly shaped art 0:17 icular surfaces 0:18 of the sacrum and ilium of the pelvis. 0:23 The sacroiliac joints are surrounded by a fibrous joint capsule, which is 0:26 relatively thin and 0:27 weak, providing limited mobility. 0:31 The fibrous capsule is lined by a synovial membrane. 0:36 The sacroiliac joint is stabilized by strong ligaments, particularly the inter 0:42 osseous sacroiliac 0:43 ligament, the key stabilizer that limits movement. 0:48 The sacroiliac joint allows only minimal motion, mainly small degrees of gl 0:53 iding and rotation, 0:56 including mutation and counter-nutation. 1:01 Sacroiliac joint motion, however, increases in pregnancy due to ligamentous lax 1:08 ity via 1:09 relaxing hormone. 1:13 While no muscles are designed to act on the sacroiliac joint to produce active 1:18 movement, 1:19 the joint is still surrounded by some of the largest and most powerful muscles 1:24 of the body. 1:26 These muscles include the erector bainae, psoas, quadratus lumborum, piriformis 1:33 , abdominal 1:34 obliques, gluteals, hamstring muscles and pelvic floor muscles, the levator ani 1:41 , and 1:42 coxigial muscles. 1:49 So let's talk more about some anatomy, particularly the anatomical differences 1:54 between the male 1:56 and female pelvis, specifically the sacroiliac joint. 2:01 So in women, the ligaments, as I mentioned, become lax during pregnancy. 2:08 These factors may make women more prone to lower back pain. 2:12 During pregnancy, the hormone relaxes and increases the mobility of the sacro 2:16 iliac joint by providing 2:17 ligament laxity for giving birth. 2:21 Women have also higher range of movements, thicker sacral cartilage, thinner 2:26 iliac cortical 2:26 bone, smaller sacroiliac joint surface area, and larger interosseus sacroiliac 2:34 ligaments, 2:35 as well as smaller anterior and posterior sacroiliac ligaments. 2:40 Remember, the interosseus sacroiliac ligaments is the most important stabilizer 2:43 of the sacroiliac 2:44 joint. 2:46 And finally, women have higher mobility, as mentioned, greater stresses, 2:50 greater loads, 2:51 and more pelvis ligament strains compared to men. 3:00 Which brings us to sacroiliac joint pain and the term sacroiliitis. 3:06 So sacroiliac joint pain differs depending on the cause, but in general, the 3:13 pain, there 3:14 are specific characteristics. 3:16 Firstly, there is this deep ache or sharp pain over the posterior superior ili 3:22 ac spine 3:22 region, often where patients point to with one finger, the 14-finger sign. 3:28 Typically, buttock pain, unilateral, so one side, but can be both sides in 3:33 inflammatory 3:34 causes of sacroiliac joint pain. 3:38 The pain commonly refers, so moves along the postural lateral thigh and the 3:45 groin. 3:46 It rarely or typically does not go below the knee, however, it may radiate to 3:51 the calf 3:52 and foot, but typically not. 3:54 And it often mimics radicular pain, but usually doesn't follow a dermatonal 4:01 pattern. 4:02 There are aggravating and easing factors, so it's worse with prolonged sitting, 4:07 standing, 4:08 rolling in bed, stairs, walking uphill, single leg loads, standing on an 4:12 affected leg, running 4:13 long strides. 4:14 A pain often occurs with transitional movements, so sit to stand, getting in 4:18 and out of a car 4:19 bending forward or moving around in bed from one side to the other, however, it 4:25 's important 4:26 that the pain itself also improves with gentle walking and movement. 4:32 And this is specifically so for inflammatory sacroiliitis, an autoimmune cause. 4:43 There are many causes of sacroiliac joint pain, the mechanism of sacroiliac 4:46 joint injury primarily 4:48 is due to a combination of axial loading and abrupt rotation. 4:54 Some causes include trauma, like falls, sports, or car collisions. 4:58 A direct jolt to the pelvis can stretch the strong sacroiliac joint ligaments 5:03 and irritate 5:04 the joint lining. 5:05 It's like a sprained angle, but at the back of the pelvis's shop, one-sided 5:09 buttock pain 5:10 worse getting up or rolling in bed. 5:14 Lumbar fusion, so when the lower spinous fuse, the sacroiliac joint becomes the 5:18 next hinge 5:19 and takes extra twisting forces. 5:22 Over time, that overload can inflame the capsule and ligaments. 5:27 Lymph length discrepancy, whether it's true or functional. 5:31 If one leg effectively runs shorter, your pelvis tilts and one sacroiliac joint 5:36 is repeatedly 5:37 stressed. 5:38 A small heel lift and gait retraining can lever the load while we strengthen 5:44 the lateral hip 5:45 and trunk muscles. 5:47 Scoliosis, so a curved or rotated spine tilts the pelvis and focuses sheer on 5:51 one sacroiliac 5:52 joint. 5:53 Then, there's overuse or training injury, so running, cutting, heavy squats, 5:59 lunges, 6:00 repeated twisting, and impact can outpace tissue capacity, irritating the long, 6:07 interosseous 6:08 sacroiliac joint ligaments. 6:14 Pregnancy and early postpartum, as I mentioned, hormones loosen the pelvic lig 6:19 aments, so 6:19 the sacroiliac joint moves more. 6:22 With extra weight and postural change, it can shear and get sore. 6:27 Fractures, it's an important mimic of sacroiliac joint pain. 6:31 In some people, especially in those who have osteoporosis or steroid use, the 6:36 sacrum can 6:37 develop insufficiency fractures that feel like sacroiliac joint pain. 6:42 Runners can also get sacral stress fractures. 6:46 Infection, so there is something called septic sacroiliac, it is rare but 6:50 urgent because 6:51 bacteria can actually seed into the sacroiliac joint. 6:56 Postpartum, bloodstream, infection, tuberculosis, in the right context, it's 7:03 severe, it's constant 7:04 pain, often with high fevers, CRP, and ESR. 7:08 Finally, sacroiliitis, now the term generally when we use it describes 7:14 inflammatory sacroiliac 7:16 joints, typically autoimmune. 7:18 So it's defined as the inflammation of one or both sacroiliac joints. 7:24 It is an important cause of sacroiliac joint pain, it is an autoimmune disease. 7:29 The key type is called ankylosing spondylitis, diagnosis typically relies on 7:34 imaging. 7:35 Characteristically, sacroiliitis is defined by radiographic changes that are 7:39 graded from 7:39 zero to four using the New York criteria. 7:43 Although these changes tend to be late findings. 7:46 Here is an example of an x-ray that shows grade four sacroiliitis with fusion 7:52 of the 7:52 sacroiliac joints and evidence of the pathonomonic dagger sign. 7:56 So those are the causes of sacroiliac joint pain. 8:05 Now let's talk about some examination techniques to diagnose it. 8:08 Now the examination for sacroiliac joint is used to assess whether low back 8:13 pain, buttock 8:15 or pelvic pain originates from the sacroiliac joint. 8:18 However, there is no single test that is highly diagnostic and the reliability 8:23 improves when 8:24 multiple positive tests are used together with interpreted alongside imaging. 8:30 So the first is called a thigh thrust or the posterior shear test. 8:35 Essentially the patient is supine, hip is flex 90 degrees and slightly adducted 8:40 . 8:40 One hand blocks the sacrum, apply a firm posterior force along the femur, 8:44 positive test is reproduction 8:47 of the patient's deep buttock sacroiliac joint pain on the tested side. 8:52 The next test is the distraction or gapping test. 8:54 So a patient is supine, hands on both anterior superior illic spines, apply 9:00 postural lateral 9:01 pressure for up to 30 seconds. 9:04 It's positive if posterior pelvic or sacroiliac joint pain occurs, not groin 9:10 pain. 9:11 The compression test is where the patient lies on their side, painful side up 9:16 and essentially 9:18 put your hands over the upper eye layer crest and you press down towards the 9:22 table. 9:23 It's positive if there is that posterior pelvic sacroiliac joint pain occurring 9:29 . 9:30 The sacral thrust is when a patient is prone, so on their belly, heel of hands 9:36 essentially 9:37 you place over the sacrum S2 to S3 and you want to deliver a ventral or an 9:43 anterior thrust, 9:44 a gentle sustained thrust and essentially it's positive if you can reproduce 9:49 the sacroiliac 9:50 joint region pain. 9:52 The Gaineslands test is when the patient is supine again near the table edge. 9:57 If flex the ipsilateral hip to the chest, you let the contralateral leg drop 10:04 off the 10:04 table into extension, stabilize the pelvis and add gentle over pressure one 10:11 side at a 10:12 time. 10:13 It's positive if the sacroiliac joint pain occurs on the down extended side, 10:20 sometimes 10:21 on the flex side. 10:23 Finally, there's the famous test or the Patrick's test. 10:27 With the patient lying on their back, supine, placed leg being tested into flex 10:33 ion abduction 10:34 and external rotation so that ankle rests on the opposite knee, making a figure 10:39 four, 10:40 stabilize the opposite pelvis and gently press down on the bend knee. 10:45 Essentially if you get groin pain, this is more hip pathology, but if you get 10:50 buttock 10:50 or posterior pelvic pain, it may suggest sacroiliac joint involvement. 11:00 So in summary, sacroiliac joint pain typically presents as deep buttock or 11:04 lower back pain 11:05 that may radiate to the groin or posterior thigh and it is often worsened by 11:11 prolonged 11:11 standing, walking or transitional movements. 11:15 Diagnosis is challenging as there is a lot of lumbar pathology or hip pathology 11:20 as well 11:20 and so even the physical examination is not definitive and you need to rely on 11:25 also imaging 11:26 if you're suspicious. 11:27 Thank you for watching.