Syncope


Syncope is defined as transient loss of consciousness due to reduced cerebral blood flow. Syncope, commonly described as “fainting,” is a symptom, not a disease, and can be classified according to the cause, the most common of which is neurocardiogenic syncope. Presyncope is feeling of fainting and patient often presents as feeling dizzy. Syncope is a transient loss of consciousness and is usually always due to a cardiovascular event such as arrhythmia or postural hypotension. Important to differentiate syncope (global cerebral hypoperfusion) with seizure (abnormal, excessive or synchronous neuronal activity in the brain) as both result in a transient loss of consciousness.
Types of true syncope
Consciousness Awareness of the environment and being able to respond to it
Syncope Transient loss of consciousness and postural tone from reduced cerebral perfusion, followed by spontaneous and full recovery
Presyncope refers to a reduction in cerebral perfusion resulting in a sensation of impending loss on consciousness, but not actually pass out. This sensation include lightheadedness, feeling of warmth, diaphoresis, visual blurring and nausea.
Transient loss of consciousness is a state of real or apparent loss of consciousness with loss of awareness, characterised by amnesia for the period of unconsciousness, abnormal motor control, loss of responsiveness and a short duration.
| Differentiating features | Seizures | Syncope |
| Age | Any | 8-15 years |
| Timing | Whenever | Day |
| Situation | Commonly during activity | Standing |
| Prodrome | Brief (twitching, hallucinations) | Long (dizziness, sweats, nausea) |
| Duration | Variable | Under 5 minutes |
| Tonic-clonic movement | Common | Rare |
| Colour change | Maybe cyanosis | Pallor |
| Injury | Common | Rare |
| Incontinent of urine | Common | Rare |
| Recovery | Drowsiness, confusion or headache | Quick Recovery |
| Aetiology of syncope | ||
| Neurally mediated syncope (Reflex syncope) | Vasovagal syncope (Neurocardiogenic) | Provoked by
|
| Situational syncope | Provoked by
| |
| Carotid sinus hypersensitivity | Provoked by
| |
| Postural (Orthostatic) hypotension | Primary autonomic failure | Lewy body disease Multiple system atrophy |
| Secondary autonomic failure | Diabetes HIV neuropathy | |
| Drug-induced (most common cause of postural hypotension) | Anti-hypertensives, diuretics, antidepressants | |
| Volume depletion | Blood loss, adrenal insufficiency, dehydration | |
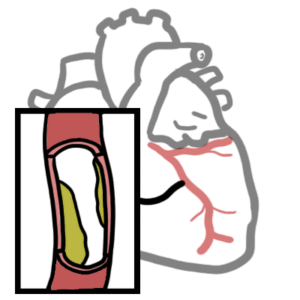
| Cardiac syncope | Arrhythmias | Bradycardia Tachycardia |
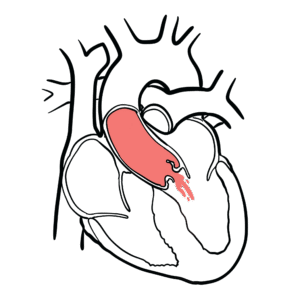
| Structural cardiac disease | Valvular heart disease Ischaemic heart disease Cardiomyopathy Pericardial disease |
Vasovagal syncope is also known as neurocardiogenic syncope. Postural hypotension is also known as orthostatic hypotension.
Syncope pentad transient loss of consciousness, loss of muscle tone, loss of responsiveness, amnesia during event, short duration, spontaneous recovery.
History
Examination
If confirmed postural hypotension review medications followed by neurological examination. If neurological exam normal consider postganglionic autonomic insufficiency.
Neurally mediated syncope (reflex syncope)
Syncope is defined as transient loss of consciousness due to reduced cerebral blood flow. Neurally mediated syncope or reflex syncope occurs when there is increases parasympathetic activity with concurrent decrease in sympathetic activity. The increase parasympathetic activity and decreased sympathetic activity (sympathetic withdrawal) causes a decreased heart rate, reduced heart contractility and vasodilation. All this causes reduces perfusion to the brain causing syncope. Three types of neurally mediated syncope which are caused by this mechanism:
For neurally mediated syncope patients can experience presyncopal symptoms such as feeling unwell, nauseated, dizzy, or tired, with yawning, blurred or ‘tunnel’ vision, or altered hearing. After their syncopal episode patients recover rapidly.
Often patient experience what called Bezold–Jarisch reflex
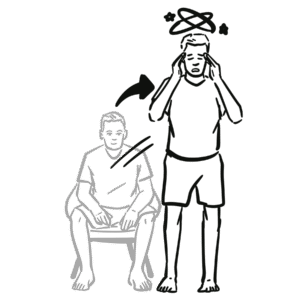
Postural Hypotension (orthostatic hypotension)
Orthostatic hypotension is an important, treatable cause of dizziness, syncope and falls. Less frequently it leads to visual disruption, dyspnea on exertion, angina and even stroke. Orthostatic hypotension also known as postural hypotension results from a failed sympathetic response when standing upright resulting in decrease venous return and cardiac output causing dizziness, syncope and/or fall.
Main mechanism of postural hypotension
Click here for more information on postural hypotension
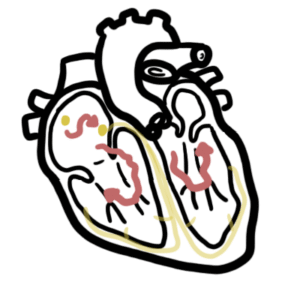
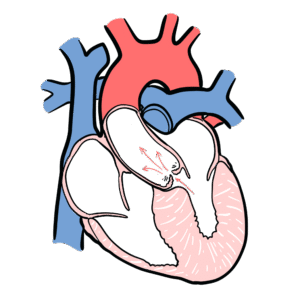
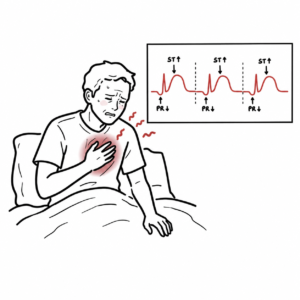
Cardiac syncope









Discussion