

Chest Pain

Overview
The most common and important cardiovascular symptom. It is also a very important symptom for the lungs and oesophagus, where the character, pattern of pain and associated symptoms differ. Initial management include oxygen, analgesia, nitrates (to rule in MI) and investigations with ECG and chest X-ray are urgent for patients who present with chest pain + grave signs and symptoms such as diaphoresis, tachycardia, hypotension, fever and sudden dyspnea. You want to rule out life-threatening causes first which are discussed below.
| CAUSES OF CHEST PAIN BY BODY SYSTEMS | ||||
| Cardiac | Respiratory | Gastrointestinal | Musculoskeletal | Psychogenic |
| Acute Coronary Syndrome | Pulmonary Embolism | Oesophageal rupture | Rib Fracture | Anxiety |
| Aortic dissection | Pneumothorax | Pneumomediastinum | Herpes Zoster | Panic attack |
| Pericarditis | Pulmonary Hypertension | Cholecystitis | Costochondritis | |
| Stable Angina | Pneumonia | GERD/GORD | ||
| Endocarditis | Lung Cancer | Peptic ulcer disease | ||
| Cardiac tamponade | Bronchiectasis | Acute Pancreatitis | ||
Types of chest pain
- Pleuritic Pain – pain from parietal pleura and endothoracic fascia (the visceral pleura is insensitive to pain). It is worse on inspiration, reflecting the stretching of inflamed parietal pleura during movement of the thorax. No relief with GTN and does not radiate.
- Pulmonary (Lung parenchymal) Pain – Dull and constant pain.
- Diaphragmatic pain – pain referred to the shoulder tips. If pain located in costal parts of the diaphragm it radiates to the abdomen.
- Chest wall (musculoskeletal) pain – It is rarely severe and incapacitating, is often bilateral, and generally is intensified by changes in body position or flexing the thorax. Confused with pleuritic pain. Tender to touch.
- Burning pain – Esophageal disease, frequently after eating. Acid reflux may worsen with recumbency.
- Cardiac pain – varies (dissecting aorta, stable angina, acute coronary syndrome and pericarditis)
Just because chest is tender on palpation does not mean the chest pain is musculoskeletal.
| Life-threatening Chest Pain Clinical Features | |||
| Conditions | Pain Feature (Acute) | Associated Signs and Symptoms | Examination |
| Aortic dissection |
|
| Prostration
Loss of pulse |
| Pulmonary Embolism |
|
| Asymmetric extremity swelling (DVT?) |
| Pneumothorax |
|
| Inspection: Asthentic habitus. Trachea deviation (only in tension pneumothorax), chest wall asymmetry (large pneumothorax)
Percussion: hyperresonant Auscultation: reduced breath sounds and reduced vocal resonance on affected side |
| Cardiac Tamponade |
|
| Inspection: Raised JVP, hepatomegaly, ascites, peripheral oedema
Palpate: impalpable apex beat Auscultation: Telltale rub that is synchronous with the heartbeat |
| Acute coronary Sydnrome (Acute MI) |
| Inspection: Previous thoracic surgery
Palpapte: Heaves/Thrills Auscultate: Tachycardia | |
| Oesophageal rupture (Boerhaave syndrome) |
|
| |
Signs and Symptoms of MI – PULSE
Persistent chest pain, Upset stomach, Lightheadedness, Shortness of breath, Excessive sweating
General Management – stabilize airway, breathing and circulation
- Oxygen
- Aspirin
- Nitrates – for angina relief
- IV access
- Pain Relief – analgesia
- Troponin and possibly other cardiac markers
Treatment Acute MI – MONAC
Morphine, Oxygen, Nitrates, Aspirin + Clopedogril
Investigation
- Full Blood count – White cell count may be elevated in any of the inflammatory or infectious aetiologies (ie. myocarditis, pericarditis, pneumonia)
- EUC
- Troponin – diagnosis of Acute MI
- D-dimer – can help rule out PE
- Chest X-ray
- ECG
- Other: B-type natriuretic peptide (heart failure), CT scan – aortic dissection and PE, Echocardiogram – pericarditis, pericardial effusion and valvular heart disease,
Troponin I elevated within 3 hours peak at 12hours and remain elevated for 7-10 days.
| Life- threatening Chest Pain Features in CXR and ECG | |||
| Conditions | Pain feature | Chest-x – ray | ECG |
| Aortic dissection | Sudden severe tearing pain often radiating to back | Widened mediastinum | Can be completely normal to ST segment elevation if the dissection involes the origin of a coronary artery |
| Pulmonary Embolism | Sudden severe pleuritic chest pain
Can worsen overtime | Westermark’s mediastinum
Hampton’s hump | “S1Q3T3” (ie, prominent S wave in lead I, Q wave in lead III, and inverted T wave in lead III) reflects right heart strain but is neither sensitive nor specific for PE |
| Pneumothorax | Sudden severe unilateral chest pain | Visceral pleural line typically identified | Normal |
| Cardiac tamponade | Anterior precordial pleuritic pain.
Worse lying supine, relieved leaning forward. Worse on inspiration | Large globular heart (Cardiac Tamponade) | Initial diffuse elevated ST segments ± depressed PR segment. 2-5 days later ST isoelectric with T wave flattening and inversion. |
| Acute coronary Sydnrome (Acute MI) | Often described as “discomfort” rather than pain
Constricting chest pain, crushing chest pain radiating to neck/shoulder | May show left ventricular hypertrophy, cardiomyopathy or previous stent/pacemaker. | ST elevation in leads associated with injured area of heart and reciprocal lead changes (depression) OR ST depression |
| Oesophageal Rupture | Depend upon the location of the perforation: | Mediastinal or free peritoneal air
Subcutaneous emphysema |
|
Approximately 90 percent of patients with aortic dissection will have some CXR abnormality. The classic findings of a widened mediastinum or aortic knob occur in up to 76 percent of patients.
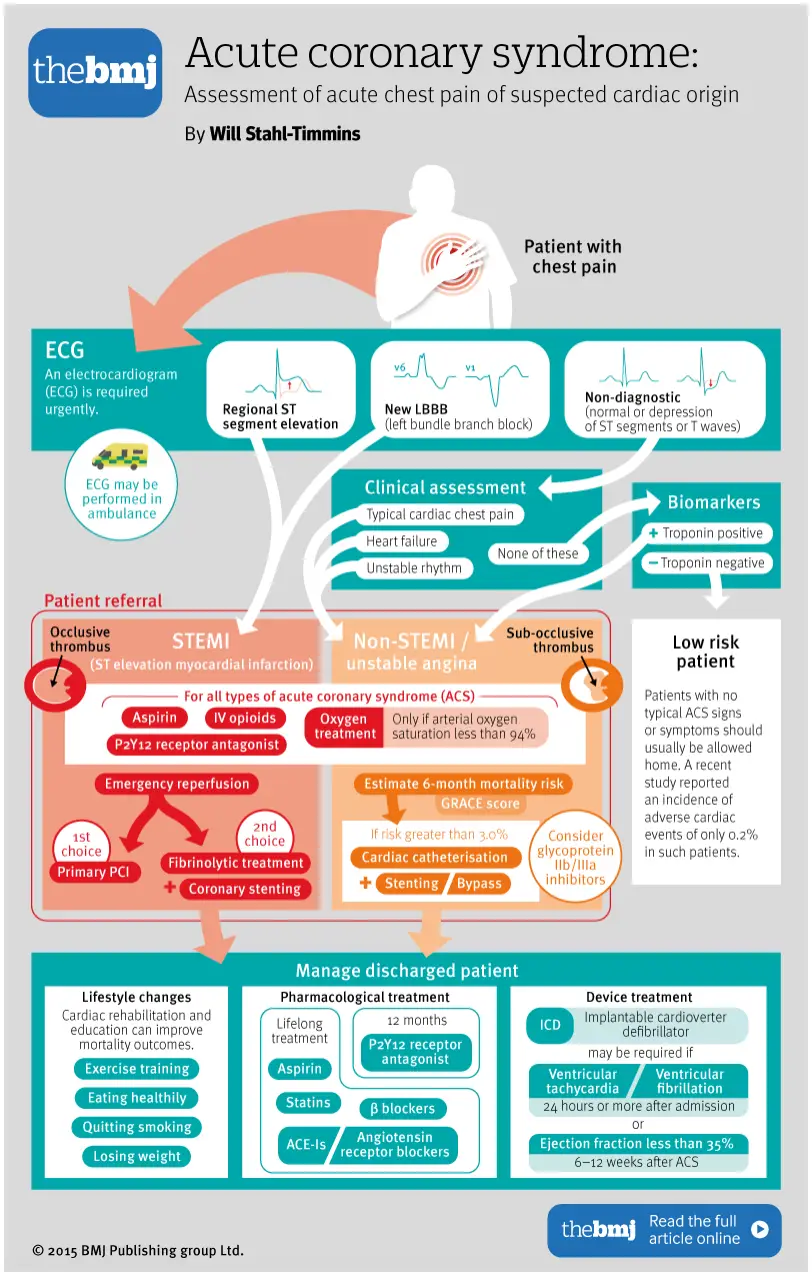
Chest Pain Management Pathway – from BMJ







Members only discussions coming soon…